
Learning objectives for this chapter
By the end of this chapter, we would like you:
- To explain the place of health observation and assessment in the nursing care cycle.
- To list and describe the three key steps involved in health observation and assessment.
- To explain the difference between signs (objective) and symptoms (subjective).
- To describe the application of clinical judgement to understand assessment data.
- To discuss cultural considerations related to health observation and assessment.
- To describe the processes involved in conducting a systematic head-to-toe assessment of a patient, including completing a primary survey and a secondary survey.
- To be able to accurately document health observation and assessment findings.
Health observation and assessment in nursing practice
|
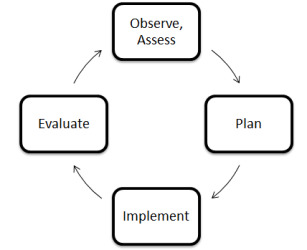
Health observation and assessment is a systematic process to collect data about a patient. This data provides information about the patient's condition, and is used to inform the care which is appropriate for that patient. Nurses undertake health observation and assessment constantly, in all clinical settings. Health observation and assessment is the first step in the nursing care cycle, illustrated in the diagram to the right: |
|
Health assessment involves three concurrent steps:

- Health History: collecting subjective data - data about a patient's symptoms. Data is collected via an interview with the patient and / or significant others. Data collected may be primary or secondary.
- Physical Examination: collecting objective data - data about a patient's signs. Data is collected via a physical examination of the patient, using techniques such as inspection, palpation, percussion and auscultation, and measurement of the vital signs and other key physical indicators.
Symptoms are what the patient subjectively experiences. Signs are what a nurse objectively observes, feels, hears or measures. In some cases, data collected during health observation and assessment may be both a symptom and a sign. For example, a client may say that she "feels sweaty" (a symptom), and the nurse observes diaphoresis (a sign).
- Documentation of Data: data collected during health observation and assessment must be documented so that it can be used to: (1) assess the patient's condition, and (2) inform the care which is appropriate for that patient. There are a variety of ways that data can be recorded. Regardless of the manner, documentation must be complete, accurate, concise, legible and free from bias.
There are a number of different types of health assessment which a nurse may undertake:
- Comprehensive health assessment: taking a detailed health history and physical examination of a client, to identify all of the person's health care issues and needs. Usually performed on admission.
- Problem-based / focused health assessment: collecting data related to a specific complaint. Common in outpatient settings.
- Rapid assessment: collecting data to provide immediate, life-sustaining intervention to a patient. Often performed in emergency care.
- Episodic / follow-up assessment: a nurse following up with a patient to collect data on a previously-identified problem. The goal is to determine how the patient has responded to care, by identifying changes in the patient's condition.
- Screening assessment: collecting data with the aim of detecting the presence of a specific disease.
The type of assessment used depends on: (1) the context, and (2) the health care issues and needs of the patient. In an acute care setting with a new client, a comprehensive health assessment is usually appropriate. However, in an emergency care setting where a patient presents with a clear, significant problem, a rapid assessment is typically more suitable.
Cultural considerations in health observation and assessment
A person's culture is far more than simply their ethnic background; it involves how they live in and perceive the world around them. People who share a culture also share values, beliefs and attitudes about various topics - including about their health. Nurses have the responsibility of providing effective care to people whose health practices, values, beliefs and attitudes may differ significantly from their own.
It is important that nurses are respectful of a diverse health practices, values, beliefs and attitudes. This involves, in part, becoming a culturally competent nurse.
Nurses are not expected to know all the health practices, values, beliefs and attitudes of all the different cultural groups they work with. They should also avoid stereotyping the people with whom they work. Rather, nurses must recognise each person as an individual. Nurses are encouraged to ask questions to understand the patient's health practices, values, beliefs and attitudes.
Conducting a systematic head-to-toe assessment and primary / secondary survey
This chapter introduces the idea of a 'head-to-toe assessment', a physical examination which enables a nurse to assess a client systematically and comprehensively from the top of their body downwards. When conducing a head-to-toe assessment, nurses assess each body system in turn, to develop a detailed overall understanding of the patient's condition.
Each nurse's approach to completing a head-to-toe assessment is unique. The only requirement for a head-to-toe assessment is that the process is systematic and comprehensive, and that no data is omitted.
Head-to-toe assessment begins with observation. The nurse should observe the patient, noting their gait, posture and ease of movement, communication ability, physical appearance and general mental alertness / orientation / thought process. This is to identify any obvious problems which may need to be addressed assessment can begin, or which may inform the focus of this health assessment.
Once a nurse has completed their observation of a patient, they can progress to completing the head-to-toe assessment. This is done in two parts:
- The primary survey, which involves assessing the patient's life-sustaining body systems.
- The secondary survey, which involves a more comprehensive assessment of the patient.
The primary survey involves four stages, which may be remembered using the 'ABCD' mnemonic:
|
A |
Airway |
This step involves assessing the patency of the airway. A nurse should observe the patient for dyspnoea, excessive upper respiratory secretions, respiratory problems such as coughing / choking, and airway trauma, etc. |
||||||||
|
B |
Breathing |
This step involves assessing the adequacy of the patient's breathing and gas exchange. The nurse should observe the patient for dyspnoea, paradoxic or asymmetrical movements of the chest wall, accessory muscle use, changes in breath sounds, cyanosis, tachycardia, etc. |
||||||||
|
C |
Circulation |
This step involves assessing the functioning of the cardiovascular system and whether the patient has adequate blood volume. The nurse should assess the quality and rate of the pulse, capillary refill time, and skin colour and temperature. |
||||||||
|
D |
Disability |
This step involves briefly assessing the patient's neurological system, including their level of consciousness. Another simple mnemonic - 'AVPU' - is used to prompt nurses during this step:
During this step of the primary survey, other disabilities - for example, obvious physical or psychological problems - may also be identified. |
The vital signs should also be measured and recorded. The nurse can then progress to the secondary survey. This involves using four key techniques:
- Inspection - assessing a part of the body by observing it.
- Palpation - assessing a part of the body by touch. The nurse may use their palmar surfaces and finger pads to determine position, texture, size, consistency, masses, fluids, crepitus, pulsations, etc.
- Percussion - assessing the contents of a space in the body by tapping it with a finger. Percussion is undertaken to evaluate the size, borders and consistency of the internal organs, to identify tenderness, and to detect the presence of fluid in a body cavity. When percussing the body, the nurse should expect to hear the following sounds:
|
Area Percussed |
Normal / Expected Sounds |
|
Lungs |
Resonant tone; loud intensity; low pitch; long duration; hollow quality. |
|
Bone, muscle |
Flat tone; soft intensity; high pitch; short duration; extremely dull quality. |
|
Viscera, liver |
Dull tone; medium intensity; medium to high pitch; medium duration; 'thud-like' quality. |
|
Stomach, gas in intestines |
Tympanic tone; loud intensity; high pitch; medium duration; 'drum-like' quality. |
|
Air trapped in lungs (e.g. in emphysema) |
Hyper-resonant tone; very loud intensity; very low pitch; longer duration; booming quality. |
- Auscultation - listening to sounds.
The nurse should assess:
|
Body Region |
Examples of Health Observation and Assessment |
|
The head and face |
|
|
The eyes |
|
|
The ears |
|
|
The nose, mouth and oropharynx |
|
|
The neck |
|
|
The upper extremities |
|
|
The posterior chest |
|
|
The anterior chest |
|
|
The abdomen |
|
|
The lower extremities |
|
|
The neurologic system |
|
|
The genitalia and rectum (if indicated) |
|
It is important that nurses comply with their organisation's policies and procedures. In order to perform an assessment using a particular technique, it is also important that nurses are appropriately trained in the correct use of that technique, and in the data it returns.
There are a range of other focused assessments which may also be completed - for example:
- Blood glucose levels.
- Blood laboratory studies.
- Comprehensive neurological evaluation.
- Diagnostic imaging studies.
- Electrocardiogram (ECG) monitoring.
- Height, weight and Body Mass Index (BMI).
- Mental health assessment.
- Neurovascular function.
- Pain assessment.
- Sensory perception.
- Skin assessment.
- Urinalysis.
It is important that nurses are familiar with any pieces of equipment which may be used in the assessment of a patient. This equipment may include (but is not limited to):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
When assessing a patient, it is important that you are organised and prepared with the equipment you need. It is important that you develop a routine, and that you practice this so you develop confidence.
Documenting health observation and assessment findings
At each stage of the assessment, it is important that nurses document, or record in written format, the data they collect. This allows data to be: (1) used to determine the patient's clinical condition and make decisions about appropriate care, and (2) communicated between different professionals involved in the care of the patient.
There are a variety of different ways that data can be recorded, and this differs between clinical settings and organisations. Regardless of how data is recorded, however, documentation must:
- Be complete, accurate, concise, legible and free from bias.
- Record facts, without the use of non-committal language.
- Be written contemporaneously, or as close to the time of collection as possible.
- Include the name, signature and designation of the nurse who created it.
- Be unaltered; if errors are made, these must be struck through with one line and initialled.
- Be kept securely, an in a way which protects the patient's right to confidentiality.
- Avoid using acronyms, abbreviations, jargon and archaic terms.
- Use short sentences and simple words.
- Involve the patient and their significant others, and use language they understand.
As stated by the National Health Service's (NHS, 2010: p. 2) CG2 - Record Keeping Guidelines, "[r]ecords must demonstrate a full account of the assessment made, the care planned and provided and actions taken, including information shared with other health professionals."
Creating and maintaining appropriate documentation is a legal, ethical and professional requirement for nurses. Health records provide evidence about the type of assessment and care patients receive. They are also important clinical tools, enabling continuity of care and effective decision-making.
Conclusion
This chapter has provided a broad introduction to health observation and assessment. It began with an overview of health observation and assessment. The processes involved in conducting a head-to-toe assessment, including a primary and secondary survey, to collect data from a patient in an accurate, comprehensive and systematic way have been described. Finally, this chapter described the correct documentation, or recording, of data collected during health observation and assessment.
Cite This Work
To export a reference to this article please select a referencing style below: