
Introduction
So far in this module, you have studied the processes involved in observing and assessing each of the major body systems. This chapter will introduce focused assessment of common issues which affect a number of the body systems concurrently: pain, mental health status and nutritional status. This chapter describes how to collect a health history, and complete a physical examination, when undertaking each of these types of focused assessments. This chapter will also explain many key considerations when assessing a patient's pain, mental health status and nutritional status, including the anatomy, physiology and types of pain, the risk factors for common mental illnesses such as anxiety and depression, the types of mental illnesses and their typical presentation, and common nutritional disorders.
Learning objectives for this chapter
By the end of this chapter, we would like you:
- To describe the fundamental anatomy and physiology of pain.
- To list the different types of pain.
- To explain how to collect a health history in the assessment of a patient's pain.
- To explain how to complete a physical examination in the assessment of a patient's pain.
- To explain the concept of mental health and mental illness.
- To explain how to collect a health history in the assessment of a patient's mental health.
- To explain how to complete a physical examination in the assessment of a patient's mental health.
- To identify the risk factors for anxiety and depression.
- To recognise the different types of mental illnesses, and their typical presentation.
- To explain how to collect a health history in the assessment of a patient's nutritional status.
- To explain how to complete a physical examination in the assessment of a patient's nutritional status.
If you need assistance with writing your essay, our professional nursing essay writing service is here to help!
Find out moreFundamental anatomy and physiology of pain
Pain is defined as "an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage" (International Association for the Study of Pain, 2016). It is a common experience for many patients presenting to health care settings in the United Kingdom. To assess - and, therefore, manage - pain effectively, it is important that nurses have a fundamental understanding of the pathophysiology of pain.
Pain is experienced through a process known as nociception. Receptor cells referred to as nociceptors detect noxious, or pain-causing, stimuli (which may be of mechanical, thermal or chemical origin). These nociceptors transmit the experience of the noxious stimuli, as an electrical impulse, to the brain. Electrical impulses are transmitted along nerve fibres with the assistance of neurotransmitters, particularly serotonin and noradrenaline. Once the electrical impulse reaches the brain, the brain can initiate a response to the pain. Pain is managed by using strategies to: (1) disrupt, or (2) block the transmission of pain-related electrical impulses to the brain.
There are many different types of pain. Pain is typically divided into: (1) nociceptive pain, associated with tissue damage, and (2) neuropathic pain, associated with nerve damage. Both types of pain may be: (1) constant (i.e. continuous), or (2) episodic (i.e. occurring at specific times). In addition, pain may also be classified as either: (1) acute, or (2) chronic. Read the information in the following table:
|
Acute Pain |
Chronic Pain |
|
|
Onset and Duration |
|
|
|
Cause |
|
|
|
Course |
|
|
|
Goals of Treatment |
|
|
It is important for nurses to remember that pain is a highly subjective experience - that is, it can be most effectively identified and described only by the person who is experiencing it. Each individual person has a different pain threshold (the point at which a noxious stimulus is perceived as pain) and a different pain tolerance (the duration or intensity of pain a person will endure before responding). How pain is experienced, understood and responded to by an individual is dependent on a variety of personal and cultural factors.
Pain - focused health history
As you have seen in previous chapters of this module, health observation and assessment involves three concurrent steps:

When assessing a patient's pain, the nurse must commence by collecting a health history. This involves collecting data about:
|
Component |
Rationale |
||||||||||||
|
Present health status |
Chronic illnesses, as these are important causes of pain. Current medications, taken to treat pre-existing pain or health problems which cause pain. The nurse should ask the patient about the efficacy of any medications taken in treating their pain. |
||||||||||||
|
Description of the pain |
As you saw in a previous chapter of this module, pain is assessed using a strategy remembered by the 'OPQRST' mnemonic:
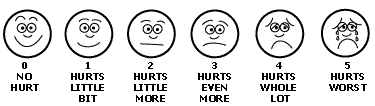
It is important for nurses to note that, on occasion, it may not be possible for a patient to describe the pain they are experiencing. This is particularly true if: (1) the patient is very young, and / or (2) the patient has a cognitive deficit. In this situation, there are a number of pain assessment tools which a nurse can use to assist the patient to describe their pain. One such tool, the 'Faces of Pain Scale', is illustrated below:
In some cases, a patient will be unable to communicate their experience of pain. This is particularly true if: (1) the patient has a particularly significant cognitive deficit, or (2) if the patient is unconscious. In this case, a nurse should be able to identify the signs of pain during their physical examination of the patient (described in greater detail following). When assessing a patient's pain, a nurse may also ask about:
|
Pain - physical examination
Once a health history of a patient's pain has been obtained, as described in the previous section of this chapter, a nurse may commence a physical examination of the patient to determine their response to the pain they experience. A stepwise process of physically examining a patient's response to pain, with normal (expected) and common abnormal findings, is presented in the following table:
|
Component |
Normal (Expected) Findings |
Abnormal Findings |
|
Observe the patient for posture and behaviour. |
The patient should be upright and relaxed. |
Any posture / behaviour to relieve pain (e.g. guarding a painful body part, rubbing / pressing a painful area); fixed movement; restless / agitated movement (e.g. wringing hands, head rocking, pacing, etc.). |
|
Observe the patient's facial expression. |
The patient should have a relaxed, neutral facial expression. |
Pain may be demonstrated by tightly closed eyes; a grimace; clenched teeth; lip-biting; wrinkled forehead, etc. |
|
Listen for sounds made by the patient. |
The patient should make no sounds other than those of normal conversation. |
Pain may be demonstrated by moaning; grunting; crying; gasping; pain may also be demonstrated if the patient makes no sound. |
|
Inspect and palpate the patient's skin for colour, temperature, moisture. |
The skin should be the expected colour for the client's ethnicity; warm; dry; elastic turgor. |
Skin may be pale; mottled; diaphoretic or very dry; unexpectedly warm. |
|
Measure the HR and BP. |
HR should be within the expected range of 60-100 beats per minute; BP should be within the expected range of 120/80mmHg. |
Sympathetic nervous system stimulation during pain may increase HR >100 beats per minute, and increase systolic BP >120mmHg. |
|
Assess RR and pattern. |
RR should be within the expected range of 10-16 breaths per minute. |
Abnormally slow and deep respirations; abnormally rapid and shallow respirations. |
|
Observe the pupillary size. |
Pupils should be 3-5 millimetres in diameter, and equal. |
Autonomic nervous system stimulation during pain may result in pupils being dilated OR constricted. |
As you saw in a previous section of this unit, once a health history and physical examination have been completed, they should be documented so that the data collected can be used to: (1) assess the patient's condition, and (2) inform the care which is appropriate for that patient. Review the following example of how the findings related to a person's experience of pain are documented:
Example
19/12/2016 - NURSING ASSESSMENT: Mrs Smith is a 55-y/o female. Complains of chronic pain in L) wrist. Medical hx: breast ca w/ bilateral mastectomy in 2006 (in remission), hypertension. Allergy: latex. Current medications: sertraline, hydrochlorothiazine, atenolol, paracetamol. SUBJECTIVE DATA: Mrs Black rates her L) wrist pain as 8/10 prior to taking paracetamol and 3/10 following paracetamol. Works as a typist, but reports difficulty continuing with work because "pain is so bad some days". OBJECTIVE DATA: Vital signs: BP 138/85, HR 88, RR 15, T° 36.6°C, SpO2 98%. Alert, orientated, cooperative. L) wrist: oedema over distal radius and medial carpals, w/o redness or heat; pain on flexion and hyperextension; strength 3/5; paraesthesia in fingers 2, 3, 4. R) wrist: no pain when performing normal range of motion activities; strength 5/5; sensation present and normal in all fingers. A MAXWELL (RN) __________________________________________________
Mental health and wellbeing
The term 'mental health' is used to describe a person's state of mind, which impacts on their ability to cope appropriately with daily stressors. It is important for nurses to remember that there are a variety of internal and external factors which determine a person's mental health; however, emotions - a key concept in the idea of mental health - are thought to be determined by the limbic system within the central nervous system. The structures of the limbic system are linked to the lobes of the cerebral cortex, surround the corpus callosum, and include the limbic lobe, the hippocampus, the amygdala, the thalamus and portions of the hypothalamus.
Activity
You are encouraged to read the National Institute for Health and Clinical Excellence's (NICE, 2011) Common Mental Health Problems: Identification and Pathways to Care guideline, or the current equivalent. This guideline can be obtained online, by searching for its title.
Mental health - focused health history
An assessment of a person's mental health is one of the few assessments where a nurse is not required to perform a physical examination of a client. This is because most of the data needed for the assessment of a person's mental health can be gathered during the health history, by talking with and observing the client. Collecting a focused health history will therefore be the focus of this section of the chapter.
When assessing a patient's mental health via a focused health history, a nurse should collect data about:
|
Component |
Rationale |
|
Present health status |
Current feelings and emotions, including about themselves, their life and their current situation, as the person's description of their feelings and emotions can provide a nurse with important information about their mental health. Current medical problems, including those which: (1) may lead to changes in mood or behaviour (e.g. endocrine disorders), or (2) may result in a person being at increased risk of mental illness (e.g. chronic painful disorders, terminal disease, etc.). Current medications, including those which: (1) are taken to manage mental illness, or (2) may lead to changes in mood and behaviour. Risk factors for mental illness, as described in detail in a following section of this chapter, which increase the likelihood that a person may develop or may have a certain mental illness. |
|
Past medical history |
History of previous mental illness, and history of coping strategies, as this can provide a nurse with important information about the types of mental illness a person may have, or may be at risk of. |
|
Family history |
Family history of mental illness (e.g. depression, anxiety, obsessive-compulsive disorder, etc.), especially among first-degree relatives, as this can provide important information about the types of disease for which a person may have a congenital risk. |
When collecting information about a person's mental health, a nurse should carefully observe the patient. The nurse should determine how the client appears and behaves, their cognitive function, their alertness and their orientation to time, place and person. These observations can provide a nurse with important information about the patient's mental status.
It is important for nurses to note that there are a variety of score tools which may be used to assess a patient's risk of certain mental illnesses. One excellent example is the Beck Depression Inventory. This tool allows a patient to score their feelings from 0 (none) to 3 (extreme) in a variety of areas, including sadness, pessimism, sense of failure, dissatisfaction, guilt, self-dislike, self-harm, social withdrawal, indecisiveness, changes in self-image, work difficulties, fatigability and anorexia. If the Beck Depression Inventory returns a score of 0-4 the person has no or minimal depression, 5-7 the person has mild depression, 8-15 the person has moderate depression, or 16+ the person has severe depression.
When using score tools to assess a patient's risk of certain mental illnesses, it is important that nurses use critical thinking to interpret the entire clinical picture of the individual patient with whom they are working. Nurses should familiarise themselves with the mental illness score tools used in the clinical setting where they work, the use of these tools in clinical practice, and how the outcomes of these tools are interpreted and used in the care of the patient.
In some cases, a person will present with a specific problem related to their mental health (e.g. depression, anxiety, etc.). Remember, nurses assess a patient's symptoms using the strategy remembered by the 'OLD CARTS' mnemonic (introduced in a previous chapter of this module). However, a symptom analysis may not be so useful when seeking information about a person's behaviour and feelings. A nurse may therefore ask more focused questions:
|
If a patient presents with… |
A nurse may ask about… |
|
Symptoms of depression, low mood. |
|
|
Symptoms of anxiety. |
|
When collecting a health history from any patient, it is important that the nurse is aware of risk factors for depression and anxiety. These are listed in the following table:
|
Risk Factors for Depression |
Risk Factors for Anxiety |
|
It is also important for a nurse to remember that a person may "develop anxiety for no apparent reason" (NHS Choices, 2016b). |
Although there is no physical examination specific to mental illness, it is important for a nurse to remember that the signs of mental illness may be identified during observation and physical examination of a client. The signs of mental illness may include (but are not limited to):
- Tense muscles, fidgeting, pacing, body tremors, perspiration; slumped posture.
- Soiled clothing / lack of hygiene.
- Changes in tone and rate of speech.
- Loss of orientation to time / place / person; failure to remember details after reorientation.
- The client has difficulty with word placement; cannot remember incorrect words.
- The client names objects incorrectly; cannot comprehend a written phrase.
- The client demonstrates a lack of judgement / reasoning.
- The client has elevated BP, HR, RR (particularly with anxiety-type disorders).
- The client's eye movements are rapid / uncoordinated.
Differential diagnosis of mental illness
When assessing a patient's mental health, there are a number of common problems and conditions a nurse may identify. Consider the conditions and their key clinical findings, outlined in the following table. This information can be useful in assisting a nurse to make a differential diagnosis of a condition affecting a person's mental health:
|
Mental Illness |
Typical Clinical Findings |
|
Depression |
Occurs when a person feels intensely sad or 'low' over a prolonged period; may be classified as 'mild', 'moderate' or 'severe'; may be described as 'melancholic' (where a person moves more slowly) and / or psychotic (where a person loses touch with reality, and experiences psychosis); leaves a person at risk of suicide. |
|
Generalised anxiety disorder |
When a person experiences intense, disproportionate and irrational anxiety over a prolonged period; may be triggered (e.g. by a phobia) or without cause; anxiety is disruptive and disabling. |
|
Panic disorder |
Panic 'attacks' (e.g. where a person becomes overwhelmed by panic / fear); attacks are usually disproportionate and irrational (but very real and distressing for the patient); may be triggered (e.g. by being in a crowded room) or occur for no apparent reason; a disorder is diagnosed when panic attacks are recurrent and disabling. |
|
Social phobia |
A person experiences an intense fear of being in the presence of / in front of / interacting with others; fears being judged, humiliated or criticised by others; actively avoids social situations. |
|
Specific phobias |
A disproportionate and irrational fear of a specific object, activity or situation; may be (1) animal-type (e.g. fear of dogs or spiders, etc.); (2) natural environment-type (e.g. fear of thunder or heights, etc.); (3) blood / injection / injury-type (e.g. fear associated with invasive medical procedures, with seeing blood, with experiencing injury, etc.); (4) situational-type (e.g. fear of elevators, bridges, driving, etc.); and / or (5) 'other' specific phobias (e.g. fear of choking); the person experiences fear and panic when exposed to their trigger. |
|
Obsessive-compulsive disorder |
When a person's anxious thoughts influence their behaviour; results in obsessions (i.e. recurrent thoughts - e.g. "I've got germs on my hands, I'm dirty") and compulsions (i.e. recurrent behaviours - e.g. repeatedly washing hands); there are many different obsessions and compulsions. |
|
Post-traumatic stress disorder (PTSD) |
Reactions a person may develop following exposure to a traumatic event (e.g. a serious accident, assault, war / torture or natural disaster, etc.); a person experiences intense fear, helplessness, horror particularly when thinking about the event; leaves a person vulnerable to depression, anxiety, addiction disorders, suicide, etc. |
|
Bipolar disorder |
When a person experiences cycles of extreme low moods (depression) and extreme high moods (mania); cycles occur over weeks / months; cycles are often disruptive and disabling. |
|
Schizophrenia |
A psychotic disorder where a person experiences a loss of contact with reality, hallucinations, delusions; caused by complex changes in brain function; leaves a person vulnerable to depression, anxiety, addiction disorders, suicide, etc. |
|
Dementia |
A disorder resulting from changes in brain structure and function; includes Alzheimer's disease, vascular dementia, Parkinson's disease, dementia with Lewy bodies, Fronto-temporal lobar degeneration, Huntington's disease and alcohol-related dementia; mostly occurs in people >65 years of age but is not unknown in younger people. |
|
Delirium |
A disturbance of consciousness with a change in cognition; develops over a short period of time; usually related to a medical condition (e.g. chronic illness, changes in metabolic balance, medication, infection, surgery or substance withdrawal, etc.); a person may be hyperactive, hypoactive or cycle between the two states. |
If you need assistance with writing your essay, our professional nursing essay writing service is here to help!
Find out moreWhen assessing a person for mental illness, it is important for nurses to remember that drug and / or alcohol intoxication can closely mimic mental illness. It is also very common for drug and / or alcohol intoxication to occur in conjunction with mental illness, as clients seek to self-medicate their mental illness. There are a variety of substances with which a person may be intoxicated:
- Alcohol (e.g. beer, wine, spirits).
- Narcotics (e.g. heroin, morphine, fentanyl).
- Stimulants (e.g. cocaine, methamphetamine).
- Depressants (e.g. alcohol, ketamine).
- Hallucinogens (e.g. phencyclidine [PCP]).
- Club drugs (e.g. ecstasy, gamma-hydroxybutyrate [GHB]).
- Inhalants (e.g. marijuana, glues, paints, petrol, aerosols).
- Prescribed medications (e.g. salicylates, acetaminophen, opiates, central nervous system [CNS] stimulants, benzodiazepines, tricyclic antidepressants, etc.).
The symptoms of intoxication vary depending on the substance taken; however, typically a patient will usually present with changes in their level of conscious, cognition, perception, affect, behaviour and motor coordination, etc. In cases of severe intoxication, a patient may be significantly compromised and present with seizures or in a coma. Although it is impossible to be familiar with the effects of all the various substances on which a patient may become intoxicated, it is important that nurses know the effects of the substances most often seen in the clinical setting and region where they work.
It is also important for a nurse to remember that neurological illness and injury can mimic mental illness. Again, neurological illness / injury can occur in conjunction with mental illness. You studied differential diagnosis of a variety of neurological conditions in detail in an earlier chapter of this module; you should revise this chapter now.
When assessing a person for mental illness, it is important for nurses to remember that mental illness is associated with much stigma in the United Kingdom.
Activity
You are encouraged to read the Mental Health Foundation's Stigma and Discrimination website, or the current equivalent. This website can be accessed online, by searching for its title.
Stigma may make a patient reluctant to seek assessment or treatment for mental illness, it may cause them to be unwilling to accept the results of a mental health assessment, and it may result in their noncompliance with a treatment regimen. Nurses must ensure they care for patients with mental illness, including during assessment, in a non-judgemental way and non-discriminative way; this is important in providing high quality care.
Assessment of nutrition
Foods and fluids are among the most basic biological needs; therefore, a nutritional assessment is an important aspect of the total health assessment of a patient. Nutritional assessment is not typically performed in isolation (unless a patient presents with a specific nutrition-related problem); rather, it is one part of the broader general assessment. The nutrition assessment includes a focused health history, and a physical examination involving anthropometric measurements and biochemical tests.
Nutrition assessment - focused health history
When assessing a patient's nutritional status, the nurse must commence by collecting a health history. This involves collecting data about:
|
Component |
Rationale |
|
Present health status |
Current illnesses, particularly those which may affect a patient's nutritional status (e.g. diabetes, cystic fibrosis, phenylketonuria, coeliac disease, renal disease, cancer, etc.). Current medications, particularly those which: (1) may affect a patient's appetite and / or capacity to digest foods, (2) may result in gastrointestinal symptoms (e.g. nausea / vomiting, satiety, constipation, diarrhoea, etc.), or (3) may be affected by certain foods. Unexplained changes in weight in the previous 6 months, as unexplained weight gain or weight loss can indicate a nutritional problem and / or another health issue. Food intolerances and / or allergies, and how these issues are managed, as this can provide a nurse with important information about a person's nutritional status. Problems obtaining, preparing or consuming foods, as these issues can result in nutrition-related health problems. Use of drugs and / or alcohol, as this can contribute significantly to nutritional deficiencies and related problems. |
|
Past medical / family history |
Past concerns about weight / problems eating, and how these issues were managed, as this can help a nurse understand how to best manage any current nutritional issues the patient is experiencing. Family history of nutritional problems (e.g. obesity, eating disorder, etc.), especially among first-degree relatives, as this can provide important information about the types of disease for which a person may have a congenital risk. |
In some cases, a person will present with a specific problem related to their nutritional status (e.g. weight loss / gain, difficulty chewing / swallowing, loss of appetite, nausea, etc.). Remember, nurses assess a patient's symptoms using the strategy remembered by the 'OLD CARTS' mnemonic (introduced in a previous chapter of this module).
When collecting a health history from a patient, it is important for a nurse to gather data about a patient's dietary intake. This usually involves a patient recalling and reporting their dietary intake over the course of one or several days, using one of the following techniques:
|
Technique |
Description |
|
24-hour recall |
The client recalls everything they have consumed in the previous 24 hours. |
|
Typical food intake |
The client describes the foods / drinks they typically consume in a day. |
|
Food diary |
The client records everything they consume in a given period (e.g. 1 week). |
|
Food frequency questionnaire |
The client indicates the frequency of intake of certain foods (e.g. number of servings per day, week, etc.). |
Once information about a patient's dietary intake has been obtained, the adequacy of their diet must be evaluated. This involves comparing the diet to the current UK national recommendations for the patient's gender and age. This step may involve the assistance of an allied health professional, such as a nutritionist or a dietician.
It is important for a nurse to realise that there are some limitations with these techniques to gather data about a patient's dietary intake. For example, it can be challenging for a patient to recall and report their intake accurately. Furthermore, such a 'snapshot' of a patient's nutritional intake may not reflect their actual intake over a longer period of time. A nurse should consider these limitations when using these techniques, and interpreting findings.
When collecting a health history from any patient, it is important that the nurse is aware of risk factors for common nutrition-related problems - including obesity, malnutrition and eating disorders. These are listed in the following table:
|
Risk Factors for Obesity |
Risk Factors for Malnutrition |
Risk Factors for Eating Disorders |
|
|
|
Nutritional assessment - physical examination
Once a health history related to a person's nutritional status has been obtained, as described in the previous section of this chapter, a nurse may commence a physical examination to further investigate a patient's nutritional status. A stepwise process of undertaking this physical examination, with normal (expected) and common abnormal findings, is presented in the following table:
|
Component |
Normal (Expected) Findings |
Abnormal Findings |
|
Measure Body Mass Index (BMI), as described in an earlier chapter. |
BMI 18.6 to 24.9 (normal weight). |
BMI <18.5 (underweight); BMI 25-29.9 (overweight); BMI >30 (obese). |
|
Assess the client's general appearance. |
The client should appear well-nourished and well-proportioned. |
Underweight or overweight. |
|
Inspect the skin surface or characteristics, hydration, lesions. |
Skin should be smooth; elastic; without lesions / cracks / bruising. |
Oedema (e.g. fluid retention); decreased skin turgor; dry skin; bruising; follicular hyperkeratosis, etc. |
|
Inspect the hair and nails or appearance, texture. |
Hair appears shinny, smooth, firm; nails are smooth, intact, firm. |
Hair is dull, falls out easily, spoon-shaped nails, etc. |
|
Inspect the eyes for surface characteristics. |
Contunctivae should be pink; free of lesions / drainage; corneas should be clear and shiny. |
Conjunctivae are pale or excessively red; eyes have Bitot's spots ('foamy' areas); xeropthalmia, etc. |
|
Inspect the oral cavity for dentition, intact mucous membranes. |
The teeth (or dentures) should be present, intact, clean; mucous membranes should be moist, pink, intact, smooth. |
Poor dentition; painful oral lesion; dry mucous membranes; pale / bright red mucous membranes, etc. |
|
Inspect and palpate the extremities for shape, size, coordinated movement, sensation. |
Well-developed muscles, bilaterally equal; muscle strength; coordinated muscle movements; full sensation. |
Muscle weakness; muscle wasting; uncoordinated muscle movements; peripheral neuropathy / paresthesia, etc. |
It is important to note that a number of laboratory tests may be used in the nutritional assessment of a patient, including:
- Serum albumin (if low, may indicate protein deficiency).
- Haemoglobin (if low, may indicate anaemia [a deficiency of iron / folate / Vitamin B12]).
- Blood glucose (if high, may indicate diabetes mellitus; if low, may indicate caloric deficiency).
- Lipid profile (if cholesterol and / or triglycerides are high, may indicate hyperlipidaemia).
Conclusion
This chapter has introduced the processes involved in the focused assessment of common issues which affect a number of the body systems concurrently: pain, mental health status and nutritional status. It described how to collect a health history, and complete a physical examination, when undertaking each of these types of focused assessments. This chapter also explained many key considerations when assessing a patient's pain, mental health status and nutritional status, including the anatomy, physiology and types of pain, the risk factors for common mental illnesses such as anxiety and depression, the types of mental illnesses and their typical presentation, and common nutritional disorders. In completing this chapter, you have equipped yourself with the knowledge and skills necessary to comprehensively assess a person's pain, mental health status and nutritional status.
If you need assistance with writing your essay, our professional nursing essay writing service is here to help!
Find out moreReflection
Now we have reached the end of this chapter, you should be able:
- To describe the fundamental anatomy and physiology of pain.
- To list the different types of pain.
- To explain how to collect a health history in the assessment of a patient's pain.
- To explain how to complete a physical examination in the assessment of a patient's pain.
- To explain the concept of mental health and mental illness.
- To explain how to collect a health history in the assessment of a patient's mental health.
- To explain how to complete a physical examination in the assessment of a patient's mental health.
- To identify the risk factors for anxiety and depression.
- To recognise the different types of mental illnesses, and their typical presentation.
- To explain how to collect a health history in the assessment of a patient's nutritional status.
- To explain how to complete a physical examination in the assessment of a patient's nutritional status.
Reference list
Cox, C. (2009). Physical Assessment for Nurses (2nd edn.). West Sussex, UK: Blackwell Publishing, Ltd.
International Association for the Study of Pain. (2016). IASP Taxonomy. Retrieved from: http://www.iasp-pain.org/Taxonomy
Jensen, S. (2014). Nursing Health Assessment: A Best Practice Approach. London, UK: Wolters Kluwer Publishing.
Mental Health Foundation. (2016). Stigma and Discrimination. Retrieved from: https://www.mentalhealth.org.uk/a-to-z/s/stigma-and-discrimination
NHS Choices. (2016a). Causes of Clinical Depression. Retrieved from: http://www.nhs.uk/Conditions/Depression/Pages/Causes.aspx
NHS Choices. (2016b). Generalised Anxiety Disorder in Adults. Retrieved from: http://www.nhs.uk/Conditions/Anxiety/Pages/Symptoms.aspx
Wilson, S.F. & Giddens, J.F. (2005). Health Assessment for Nursing Practice (4th edn.). St Louis, MI: Mosby Elsevier.
Cite This Work
To export a reference to this article please select a referencing style below: