
Introduction
Diabetes is an issue that continues to grow and plague the United States. According to the American Diabetes Association, diabetes was the seventh leading cause of death in 2015 (ADA 2015). The number of people who have received a diabetes diagnoses increased from 1.6 million in 1958 to 12.1 million in 2000 and further increased to 30.3 million in 2015 (Engelgau 2004). The CDC (2017) estimated that 1.5 million new cases of diabetes (6.7 per 1,000 persons) were diagnosed among U.S. adults aged 18 years or older in 2015 (CDC 2017). This increase of new cases may be caused by several factors: changes in diagnostic criteria, improved or enhanced detection, decreasing mortality, and changes in demographic characteristics of the population (Engelgau 2004). Diabetes is also a very costly problem; in 2017, diabetes cost the United States a total of $327 million in health care (ADA 2015). The high costs of diabetes lead to external costs such as higher insurance costs.
Obesity is known as a major risk factor for type 2 diabetes because increases in diabetes have been linked to increases in obesity. Previous literature has shown that physical inactivity is linked to weight gain. Simultaneously, there is evidence that physical inactivity directly contributes to rising diabetes rates. 12% of clinically diagnosed diabetes and hypertension cases can be attributed to physical inactivity (Colditz). Physical inactivity leads to significant weight gain and rapidly induces insulin resistance (Strasser 2013). This study contributes to the previous literature estimating the direct effect of weekly physical inactivity on state-specific diabetes rates where overweight and obesity prevalence are held constant.
Literature Review
Physical inactivity in the United States is high and is responsible for roughly 400,000 deaths annually. It has been previously determined that physical inactivity increases with age, however, there has been a recent trend of diabetes emerging at younger ages (Gordon-Larsen 2004). Kruger found that the prevalence of physical inactivity declined significantly, from 29.8% in 1994 to 23.7% in 2004 (Kruger 2004).
Previous studies show that increases in physical activity directly correlate to a decline in the diabetes rate. Helmrich (1991) used a proportional-hazards regression model to test for the independence of association between physical activity and the development of type 2 diabetes in American men over a 14-year period. Age, BMI, and year of diabetes diagnosis were entered into the model as continuous variables while history of hypertension and parental history of diabetes were inputted as dummy variables. This study found that the incidence rate of diabetes decreased by 6% for every increment of 500 kcal per week in physical activity (Helmrich).
Another study by BMJ Journals found that sedentary behaviors (physical inactivity) are positively associated with risk of type 2 diabetes through multiethnic analyses and were influenced by race/ethnicity (Joseph). This study concluded that leisure sedentary behavior on type 2 diabetic risk remained significant after full adjustment including BMI (Joseph 2016).
An international study by C. Oggioni (2014) used multilinear regression model to test whether physical inactivity influenced diabetes rates globally. The study concluded that 1% increase in prevalence of physical inactivity would predict a 0.40% increase in worldwide diabetes prevalence. The analysis indicated that the prevalence of diabetes may double over the next two decades if worldwide physical inactivity prevalence happened to rise annually by approximately 1% (Oggioni 2014).
Empirical Model
Linear regression is used to estimate the potential connection between state diabetes rates and physical inactivity. In this paper, we estimate the following regression model:
Diabetes Rate = + 1No Activity + 2Soda + 3Income + 4Uninsured + 5Region + 6Obesity + u
The dependent variable in this model, diabetes rates, measures the percent of adults who have diabetes. Physical inactivity (No Activity) measures the percentage of the population that does not engage in leisure-time physical activity.
The Soda variable measures the percentage of the population that consumes one or more sugar-sweetened beverage per day. Income variables include the proportion of the state population that falls below the federal poverty line and median income for each state. Uninsured variable measures the proportion of the state population that does not have health insurance. Obesity rate measures the proportion of the population that is either overweight or obese. Lastly, we control for geographic region- we excluded the South.
Data
This study uses 2014-2017 publicly available state-level data. Data sources for state diabetes rates, obesity rates, soda consumption, and physical inactivity are based on the Behavioral Risk Factor Surveillance System (BRFSS) an ongoing, state-based, random-digit-dialed telephone survey of non-institutionalized civilian adults aged 18 years and older. Information about the BRFSS is available at http://www.cdc.gov/brfss/index.html.
Dependent variable defines the diabetes rate as percent of adults who have diabetes. Independent variable of interest measures prevalence physical inactivity among adults by state. The rate shows proportion of adults who do not participate in any leisure-time physical activity. BRFSS data is self-reported and defines physical inactivity as not meeting the 2008 physical activity guidelines for Americans – not meeting 150 mins of aerobic activity, or 75 mins of vigorous-intensity, or an equivalent combination of both per week.
Obesity rate is defined as percentage of adults in a state who are either overweight or obese. An adult who has a BMI between 25 and 29.9 is considered overweight. An adult who has a BMI of 30 or higher is considered obese. In this study we use state obesity rates as reported by the CDC.
State characteristics include poverty rate (percent of the population at or below poverty), annual median income, and proportion of the state population that is uninsured. All state characteristics were obtained for 2016 from the Kaiser Family Foundation.
Table 1 below presents descriptive statistics.
Table 1. Descriptive Statistics

Table 1 above shows a wide variance in diabetes rates across states. Diabetes prevalence ranged from 7.1% in Utah to 15.2% in West Virginia. The average of diabetes prevalence was 10.51%. Our variable of interest, physical inactivity per week, ranged from 16.5% in Colorado to 35.1% in Tennessee and West Virginia with the average percent of inactive adults being 25.7%.
Empirical Results
Regression results in Table 2 show that physical inactivity is an important determining factor of state diabetes rates. Higher rates of physical inactivity lead to higher state diabetes rates. When the weekly physical inactivity rate increases by 1%, state diabetes rates increase by .1760% (p-value<0.05)
Table 2: Regression Results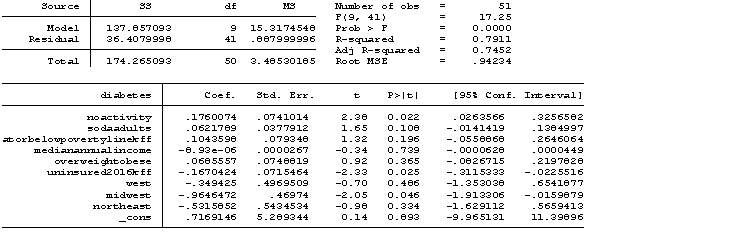
R2, the coefficient of determination, exhibits how much variation in state diabetes rates can be associated to variations in our independent variables. Shown in Table 2, 79.52% of the data can be explained by our regression model. While this accounts for the majority of variation in state diabetes rates, it is not high enough to correlate all variation in state diabetes rates. As a consequence, this model may provide useful insight to the factors contributing to state diabetes rates, but it does not provide a complete, comprehensive list of all independent variables that surround state diabetes rates.
Other important determinants of state diabetes rates include insurance and regional variables. Higher insurance rates increase diabetes diagnoses, so states with higher uninsurance rates record fewer diabetes cases (p-value<0.05). The model also finds that states in the Midwest have lower diabetes rates than states in the South (p-value<0.05)
Conclusions and Policy Implications
The empirical results show that physical inactivity is a significant driver of state diabetes rates. Creating policy to increase public physical activity should be an important target for health care officials as a potential way to decrease diabetes rates as well as obesity rates. Keeping this in mind, policy makers should: normalize conversation about physical activity at the doctor, create or extend access to more places for physical activity in communities, and investigate methods to help educate people about the many benefits of physical activity. Normalizing discussion of physical activity every time a patient goes to the doctor will help to promote the idea that physical activity is extremely important and would hopefully lead to a better understanding of the consequences of physical inactivity. Creating or extending access to physical activity centers in communities as well as educating adults on where to find places to be physically active will simply help/motivate adults to become more active. Lastly, researching ways to educate people on the negative consequences will hopefully lead to adults becoming more physically active.
Unfortunately, the results from this study are not without limitations. Diabetes, physical inactivity, and BMI were self-reported. Self-reporting may lead to error and bias in our results. Another limitation is that the sample sizes of physical inactivity is unknown; while this does not imply low causality in our model, a larger sample would better predict regression values. Also, in areas with high uninsurance rates, cases of diabetes may go undiagnosed.
References
- ADA 2015. “Statistics About Diabetes”. Available at: https://www.diabetes.org/resources/statistics/statistics-about-diabetes
- CDC 2017. National Diabetes Statistics Report. Available at: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
- Colditz, Graham A. “Economic Costs of Obesity and Inactivity : Medicine & Science in Sports & Exercise.” LWW, 1999, journals.lww.com/acsm-msse/Fulltext/1999/11001/Economic_costs_of_obesity_and_inactivity.26.aspx.
- Engelgau, Michael M., et al. “The Evolving Diabetes Burden in the United States.” Annals of Internal Medicine, American College of Physicians, 1 June 2004, annals.org/aim/fullarticle/717516/evolving-diabetes-burden-united-states.
- Gordon-Larsen, Penny. “Longitudinal physical activity and sedentary behavior trends.” APJM, 2004, https://www.ajpmonline.org/article/S0749-3797(04)00183-7/fulltext
- Helmrich, Susan P. “Physical Activity and Reduced Occurrence of Non-Insulin-Dependent Diabetes Mellitus: NEJM.” New England Journal of Medicine. 1991. 18 Sept. 2019 <https://www.nejm.org/doi/full/10.1056/NEJM199107183250302>.
- Joseph, Joshua J et al. “Physical activity, sedentary behaviors and the incidence of type 2 diabetes mellitus: The Multi-Ethnic Study of Atherosclerosis (MESA).” BMJ Open Diabetes Research & Care. 01 June 2016. BMJ Specialist Journals. 18 Sept. 2019 <https://drc.bmj.com/content/4/1/e000185#request-permissions>.
- Kruger, J. “Welcome to CAB Direct.” CAB Direct, 2004, www.cabdirect.org/cabdirect/abstract/20053187248.
- Oggioni, Clio et al. “Shifts in population dietary patterns and physical inactivity as determinants of global trends in the prevalence of diabetes: An ecological analysis.” Science Direct. Oct. 2014. 18 Sept. 2019 <https://www.sciencedirect.com/science/article/pii/S0939475314001689#!>.
- Strasser, Barbara. “Physical Activity in Obesity and Metabolic Syndrome.” Annals of the New York Academy of Sciences, Blackwell Publishing Ltd, Apr. 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3715111/.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "chronic illness"
Chronic illnesses are non-communicable diseases which develop gradually over time. They generally cannot be solved instinctively and are barely to be cured ultimately. In most cases, chronic illnesses are more likely to be insidious where the patients have mild or no symptoms.
Related Articles
