The skill that I will reflect on in this essay is the administration of an intramuscular Injection (IM). An IM is an injection deep into a muscle (Dougherty & Lister, 2008). This route is often chosen for its quick absorption rate and often medication cannot be given via other routes. The reason I have chosen to reflect on this skill is because I have had many opportunities to perform this skill, and at my current practice placement this is the most commonly used method of drug administration. I have undertook many IMs at this placement but I am going to reflect on the first one I undertook which was the administration of Hydroxocobalamin commonly known as vitamin B12 (BNF, 2007)
Description
During a morning clinic with the practice nurse, I was asked if I would like to administer an IM on the next patient, which was a 26 year old lady who has been suffering from crohn’s disease which can cause B12 deficiency due to lack of vitamin and mineral absorption (NACC, 2007). I agreed and she briefly went through with me how to do an IM as it had been a while since I had last done one. I called the patient in and asked her to sit down. The patient had come in for her first injection of B12. I chatted to the patient asking her how she was and if she had any concerns. I then gained consent asking her if it was ok for me as a student to administer it under the supervision of the practice nurse. The patient responded with “you have got to learn” I then prepared the equipment which included two needles, a sharps box, a piece of gauze and the medication. I checked the prescription with the practice nurse, and then checked the ampoule against the prescription. I then drew up the medication with one needle disposing of it in the sharps box and attached the other needle. I then proceeded to administer the medication, after completing the procedure I disposed of the needle in the sharps box and documented it in the patient’s notes. After the patient had left the nurse explained to me I had done it all correct except I had gone in too far so if the needle broke it would be hard to get it out and that I didn’t aspirate to check if I had gone into a vein.
Thoughts and feelings
After I was asked if I wanted to do the IM I felt very anxious as it had been more than 6 months since the last time I had administered one. But she explained the procedure to me which relieved some of my anxiety. When I first met the patient I was feeling allot more nervous as the patient was roughly my age and I haven’t had much experience of caring for the younger person. After the procedure when I was told I was wrong for not aspirating I felt annoyed as I was sure I had read that aspirating was no longer necessary.
Evaluation
Overall I feel that the clinical skill went well as a whole. I followed the instructions from my mentor and what the research has suggested other than feeling a little anxious I performed the skill confidently and correctly. What I feel was bad about the experience is with my communication, which reflecting on I believe was lacking. I communicated with the patient prior to the skill and after the skill, but during I felt I almost forgot there was a patient on the end of the needle. I was so focused on getting the skill right and not causing any pain I didn’t talk to the patient throughout the whole thing. Another point that I feel was bad is, I forgot to wear an apron. My mentor never mentioned anything about this although I do feel I should have worn one as it’s an aseptic technique and its part of the (DOH, 2006) guidelines.
Analysis
The reason why an IM injection was chosen is because B12 can only be administered via IM (BNF, 2007). I gained informed consent off the patient as this is part the NMC guidelines. (NMC, 2008) As patients have the right to decline treatment. After gaining consent, I then checked the medication against the patients chart to ascertain the following: Drug, Dose, date, route, the validity of the prescription and the doctor’s signature. This is done to make sure the patient receives the correct drug and dose (NMC, 2008) I then washed my hands using Ayliffes six step technique to reduce the risk of infection and put gloves on as part of DOH 2007 Guidelines . The site that I chose was the mid deltoid site. Hunt (2008) Suggests that this is the best site to use as it’s easy to access whether the patient is sitting, standing or lying down, it also has the advantage of being away from major nerves and blood vessels. Although Roger (2000) states that only 2ml at most can be injected into the deltoid. I was able to proceed with this site as B12 comes in a 1ml dose (BNF, 2007). I asked her if she would prefer to sit or lie down, she said she rather sit, this was ok with me as I am not very tall and found this a comfortable position for me. As the patient was wearing a short sleeve top I asked her to move it up slightly instead of removing it thus allowing her to maintain her privacy and dignity. I then assessed the injection site for suitability checking for any signs of infection, oedema or lesions. This is done to promote the effectiveness of administration and reduce the risk of cross infection (Woorkman, 1999). Holding the needle at a 90 degree angle it is quickly pushed into the muscle. Workman 1999 says this ensures good muscle penetration. I inserted the needle leaving approximately 1/2cm exposed as Workman, (1999) says this makes removing it easier should it break off. At this point I decided not to aspirate as per research (DOH, 2006). After inserting the needle I allowed it to remain there for 10 seconds. As Woorkman (1999) suggest that leaving in situ for 10 seconds allows the medication to diffuse into the tissues. After 10 seconds had past I swiftly removed the needle and applied pressure according to Dougherty & Lister (2008) this helps prevent the formation of a haematoma. Immediately after carrying out the skill I disposed of the needle into a rigid sharps container. To ensure health and safety is maintained and the used sharps don’t present a danger to me or other staff members as stated by MRHA (2004). After the procedure I documented it within the patient’s notes as per NMC guidelines and to provide a point of reference if there ever was a query regarding the treatment and to prevent duplicate administration (NMC, Guide lines for records and record keeping, 2005). After the skill I discussed with my mentor that recent evidence suggest that aspirating is unnecessary. According to Workman (1999) the reason for aspirating is to confirm that the needle is in the correct position and to make sure that it has not gone into a vein. The most recent and up to date evidence, says that aspiration is only necessary if using the dorsogluteal site to check for gluteal artery entry (Hunter, 2008). But official guidance from the World Health Organisation and the Department of Health (DOH, 2006) (WHO, 2004) suggest that this site should no longer be used, thus making aspiration unnecessary. By not aspirating it makes the procedure simpler and less chance of adverse events. Furthermore pharmaceutical companies are making less caustic preparations and in smaller volumes. I discussed this with my mentor and she agreed but stated that it is PCT policy to aspirate, and she would have to continue to follow this practice until the policy was amended.
Conclusion
Using the Gibbs model of reflection has allowed me to thoroughly analyse the event and allowed me to explore my feelings. I have found out despite the evidence being constantly up to date that not all practitioners knowledge is as up to date, and that trusts are equally as slow to adopt new ideas within their policies and that nurses are governed by policy more than current research. I have also learned that there is a great deal of evidence behind such what on the outside seems to be a simple technique and what I thought I was doing correctly may not always be the case.
Action plan
I do not doubt I will be carrying out IMs for a long time in my career. I will not be doing much differently in the future as the evidence is underpinning my practice. I will not put the needle in as far as I did on this occasion. In the future I will continue not to aspirate, unless local policy indicates otherwise. In addition I will communicate with the patient throughout the entire skill and not just at the start and end of. What’s more from this event I have realised that learning never stops and what I know now may not be relevant tomorrow.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gibbs reflective cycle"
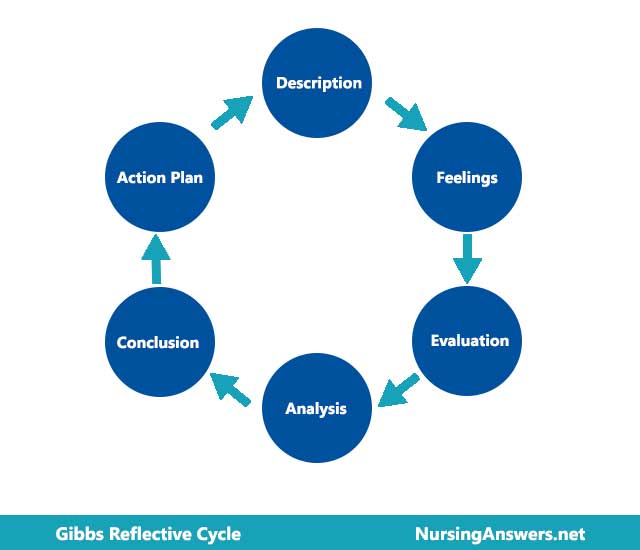
Gibbs' Reflective Cycle was developed by Graham Gibbs in 1988 to give structure to learning from experiences. It offers a framework for examining experiences, and given its cyclic nature lends itself particularly well to repeated experiences, allowing you to learn and plan from things that either went well or didn’t go well. It covers 6 stages.
Related Articles