PREPARATION FOR PROFESSIONAL PRACTICE
Part 1
The following assignment will discuss the importance of managerial delegation in practice. The learning outcomes I shall cover in this essay are to critically analyse the concepts of professional and inter-professional collaboration. I shall also demonstrate accountability and responsibility in managing the delivery of care. I shall also critically reflect upon my own strengths and weaknesses in relation to leadership qualities, management skills, communication skills and evidence based practice. All those aspects will be examined on the basis of a scenario.
The scenario concerns a patient called Betty, who was due in for admission by police escort and I asked a qualified member of staff to undertake the admission. However it became apparent that the patient was drunk upon arrival for admission. I felt inexperienced to deal with this and I recognised the need to resort to policy, legal, ethical and safety issues surrounding my delegation and decision-making before the admission could proceed. I discovered that there was no policy in respect of admittance of a drunken patient. For that reason I recognised the need to seek guidance from more experienced team members as patient safety was a concern. The good part of this experience was that I felt supported by more experienced staff members. After discussions, I felt that the admission was manageable and would not cause any safety issues in respect of patient care. I changed my decision and asked the qualified staff member to orientate the patient to the ward. Rather than asking the nursing assistant who I felt did not have the theoretical knowledge of substance misuse or appropriate skills to deal competently with the situation on this occasion. I could have refused the admission due to lack of policy guidance and if the situation arose again, I would judge the situation on its risk to patient safety and care. This scenario shows that during the course of a workday, a nurse makes decisions of many kinds, these are not trivial decisions; they involve a patient’s well-being, so it is important that as a nurse my decisions are good ones. I believe my PDP has helped me identify weaknesses as learning needs, enabling me to address these areas during practice, gaining more skills and benefiting my nursing career, patients and prospective employers. Some nurses criticise PDP’s for negatively highlighting areas of poor performance (Wilson et al 2009), others believe they positively acknowledge the nurses strengths and constructively recognise areas of improvement (Evans 2003). Policy changes and changes in nursing practice (The NHS Plan 2000, National Service Framework for Older People 1999, Making A Difference 1999, NMC 2002) means the nurses role has changed. The nurse needs to delegate tasks to enable all the daily tasks to be completed. Actually the above scenario contains aspects of leadership, management and delegation. It would therefore be important to examine those aspects and look at the differences between them.
In a transformational style, one identifies a problem, and works collaboratively with other staff to find a solution. There is an element of unpredictability as well, which empowers the nurse for the future (Faugier et al 2002). Leadership goes also with authority, influence and power (Jooste, 2004). Influence plays a more important role as a leader should be able to motivate, negotiate, and persuade instead of simply wielding power. This influence is to model by example, to build caring relationships, and mentor by instruction (Jooste, 2004). Leadership goes also along with management, but confusion prevails about these two notions (Marquis et al 2009). The differences lie in the roles of the leader and a manager as made clear by (Hughes et al 2006) in the following distinctions: “managers administer, leaders innovate; managers maintain, leaders develop; managers control, leaders inspire; managers have a short-term view, leaders have a long-term view; managers ask how and when, leaders ask what and why; managers initiate, leaders originate; managers accept the status quo, leaders challenge it.” Managerial delegation is one aspect nurses have to very careful about. As a matter of fact, delegation is the turning over of both authority and responsibility for doing work duties to a subordinate, but additionally explaining the ‘what’ and ‘why’ of a selected job, whilst leaving the ‘how’ up to the subordinates (Coburn et al 2006). It is “is the process by which you (the delegator) allocate clinical or non-clinical treatment or care to a competent person (the delegate). You will remain responsible for the overall management of the service user, and accountable for your decision to delegate. You will not be accountable for the decisions and actions of the delegate” (Wales (NLIAH), 2010). This brings about a new level of professional decision-making and the nurse as a person with managerial skills and delegation (Thomas et al 2009). As part of my management placement I would learn of my managerial and delegation duties for the day during handover when I would identify what tasks needed doing. Following this I would check the ward diary and the doctor’s book to see what tasks I needed to delegate to ensure that all the patients were cared for safely.
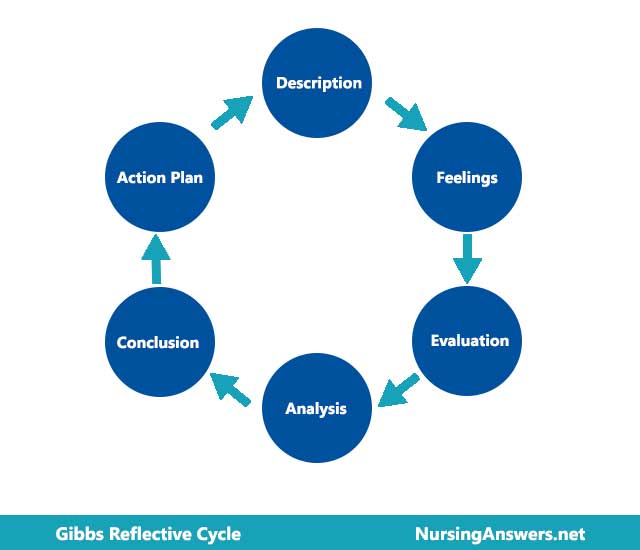
Evidence suggests, many student nurses and newly qualified nurses feel unskilled at delegation due to limited educational training and inexperience in the work place (Johnson et al 2006). On placement I felt ill prepared to delegate to staff members for these reasons, however I recognised that the best way to develop this skill would be through experiential learning. Delegation is a skill, which (Johnson et al 2006) argues is better acquired through experiential learning than lectures. (Kolb 1984) describes the experiential learning cycle as experience, reflection, generalising and planning. (Simon et al 2009) and (Parsons 2009) argue that delegation should not be purely experiential as research suggests educational sessions have resulted in knowledge and confidence for decision-making (Conger 1993). Making a Difference (DOH 1999) supports both views, as do I. I found it hard to determine what can and should be delegated in case I compromised patient care. I over came this by using a theoretical framework alongside experiential learning. I critically analysed two frameworks. The first being the Four Rights of Delegation: Right task, Right person, Right communication and Right feedback (Hansten et al 2004). The second model was (Conger’s 1993); it is called delegation Decision-making Model, which addresses three areas, task analysis, problem identification and selecting the right team member for the job. However I rejected Conger’s model, as I perceived it as being flawed for the fact that it does not include feedback. Each time a task was delegated the staff member was asked to give feedback, so when they had completed their task, a written record documenting what had occurred, this way I could be sure that the patient had received the care needed. This written record can be confirmation that the task delegated has been started and finish to the instruction which I had delegated to the delegate. Any difficulties during the task which the delegate acknowledges can be further examined and future recommendations can be put in place for future practice (Warner 2008). To delegate successfully the student nurse needs to develop an understanding of team members’ job descriptions, job expectations and skills training; otherwise patient care could suffer (Thomas et al 2009). Nurses must be very careful when delegating someone, and they have to keep in mind that there are accountable. Perhaps the best way to understand this issue would be to quote from the (Nursing and Midwifery Council 2008) on what it says about the delegator’s accountability: “If the nurse or midwife is delegating care to another professional, health care support staff, carer or relative, they must delegate effectively and are accountable for the appropriateness of the delegation. The Code requires that nurses and midwives must: establish that anyone they delegate to be able to carry out their instructions; confirm that the outcome of any delegated task meets required standards and make sure that everyone they are responsible for is supervised and supported (Tomey et al 2009). I reflected upon the above experiences via self-reflection, peer and clinical supervision with my mentor. I decided that communicating more effectively to staff members was crucial to my ability to delegate better. I believed that my good communication skills were invaluable to me when learning how to delegate. (Parkman et al 2004) states that “effective communication is a fundamental asset to successful delegation”. Evidence has shown that good communication skills by the student nurse will enable them to be more successful in delegating resulting in higher levels of job satisfaction as it empowers all team members (Parsons et al 2009). Using (Gibbs Reflective Cycle 1988) to reflect and evaluate my delegation experiences and in turns the quality of care provided for patients has helped me to become more self aware in my actions. (Cook 2001) states that “when the student nurse becomes aware of these things, it impacts positively on the quality of care, therapeutic communication and relationship with the patient” (Cook 2000). I have learnt that there are barriers to reflection. (Newell et al 2008) and (Jones et al 2008), criticize the idea of reflection arguing that it is a flawed process due to an inaccurate recall of memory and hindsight bias. (Richardson et al 2002) argues that it theorise actions in hindsight therefore devaluing the skill of responding intuitively to a patient. As such this could affect the quality of care given to the patient. But as with everything new challenges will always occur. One such challenge which can occur on a daily basis is when one of my delegation requests is contested due to a conflict of personalities. These conflicts of personalities can be shown in many ways such as ageism and gender. The older delegatee can sometimes show a condescending demeanour and display a patronizing superior attitude and a reticent to taking tasks from a younger newly qualified nurse. It is hard for the newly qualified nurse to point out any mistakes to someone older with many years of experience (Nursing Times 2011). Equally it is difficult when allocating a task to a member of staff who resents being told what to do by the opposite sex. When these barriers occur it is of great value for me to reflect on my practical and theoretical skills learned. With these skills learned, I know I have the confidence to meet any challenges and incidences which I can expect to meet on a daily basis. In general, as a newly qualified nurse giving delegation tasks, the nurse has to display strength in his/her personality (Doyle et al 2006). Any frailty within the newly qualified nurse’s character will soon be exposed by the delegate and advantages can be taken. Such advantages could include taking short cuts in the tasks delegated, or giving the task to someone else without firstly notifying the delegator.
In conclusion I feel I have grown personally, professionally and evidence of this can be seen through the achievement of NMC (2002) outcome competencies, PPS, witness statements, portfolio, profile, reflection, peer and clinical supervision. I feel that I have faced up to this challenging task and whilst learning to some degree through trial and error, I feel have succeeded in gaining delegation skills, because I have combined communication skills, theory and practice, with safe practice as my priority.
Part 2
PREPARATION FOR PROFESSIONAL PRACTICE
Part Two
Drug Management
For part two, I will be using a personal development plan (PDP). By using my personal development plan coupled with the smarter framework I will have a greater chance to envisage my personal development plan. The SMARTER framework will be used in order to judge the components of my goals. See: Appendix 1
I shall focus on one part of my PDP, which I feel less confident in and that is my medication administration skills, coupled with my NHS trust’s policy on their Principles of Safe Administration of Medicines. I shall suggest ways in which I can overcome problems I have in this area. My strengths and weaknesses can be seen in appendix 5. See: Appendix 5
Some nurses criticise PDP’s for negatively highlighting areas of poor performance (Wilson 2002), others believe they positively acknowledge the nurses strengths and constructively recognise areas of improvement (Evans 2003). I believe my PDP has helped me identify weaknesses as learning needs, enabling me to address these areas during practice, gaining more skills and benefiting my nursing career, patients and prospective employer. The contents of my PDP include the prioritisation of 5 key areas for improvement, which I feel I need further knowledge and learning about, these areas are: Drug Management, IT, administration, Chairing meetings and infection control. I have set a 3 months goal in order to improve my knowledge and understanding of these areas of deficit. The way for me to achieve my goals could include such ways as Reading professional journals like British Medical Journal, Nursing standard and Nursing times, couching by IPT members, shadowing and learning form the professionals, ward resources and using the hospitals own nursing library. For an outline of my PDP please see: Appendix 2
As well as a PDP it is important that I maintain a reflective Diary, noting important events relevant for further investigation. See: Appendix 3
I have always been apprehensive when the time comes to administer the medication. I had read and heard so many bad incidents in the press and TV when fatalities had occurred due to incorrect medication being administered. Because of these fears, I have always tried to include within my PDP any incidents or information concerning the administration of medications. I am aware that each NHS trust has their own policies on the safe administration of medications. While researching the policies of my local trust, I came upon the following policies which I feel will be beneficial to improving my knowledge on the safe administration of drugs. Registered nurses in exercising their professional accountability in the safe administration of drugs must comply with the 10 R’s as listed in the trusts drugs Policy (East London NHS) See: Appendix 4
A prescribed medicine is the most frequently provided treatment for patients in the NHS and although standards for medicines prescribing, dispensing and administration are high in this country, mistakes do occur (DoH, 2004). There has been growing awareness of the causes of medicines incidents. The publication of ‘An Organisation with a Memory’ (DoH, 2000) demonstrated the government’s commitment to improving the safety of patient care with the clear aim to reduce the number of incidents of serious medicines incidents by 40 %, (Courtenay et al 2009). As a result of these facts and the government initiatives it is essential that the Trust has a supportive and clear process to improve the practice of the administration of medicines. In their review of Medicines Management, the Healthcare Commissions (State of Healthcare 2007) reported that trusts need appropriate controls to ensure that medicines-related risks are minimised (Healthcare Commission 2007). The report from the National Patient Safety Agency (NPSA), ‘Safety in doses: medicines safety incidents in the NHS’ (NPSA, 2007) outlining seven key actions for trusts to implement to improve patient safety and improve staff skills and competencies. The Nurse and Midwifery Council (NMC) Standards for Medicine Management (NMC, 2007) encourage the immediate reporting of incidents.
In order for registered nurses to keep their registration the NMC has compiled a test called (Prep) post registration education and practice. In order for nurses to achieve success in this test they must show that they have completed 35 hours of learning in relationship to the area of practice for every 3 years. The newly registered nurse must keep a (PPP) personal professional profile which will record their ongoing learning achievements (NMC) 2. The purpose of a (PPP) is so that the nurse can have a record of their achievements and it can be a source of reference. TheNursingandMidwiferyCouncil,thenursinggoverningbody,expectsall
Nursesto:acknowledgeanylimitsofpersonalknowledge, skills and take steps to remedy any relevant deficits to meet the needs of patients (NMC scope of Professional Practice).
AspartoftheNMCrequirementsforregistration,allnursesarerequiredtokeepa
Professionalportfolio.Thisrecordslearningandskillacquisitionandintegrationof thisprofessionaldevelopmentintopractice.InspectionofthisportfoliodocumentcanberequestedbytheNMCatanytime,asthisprovidesevidenceofmeetingprofessionalstandards. Having set my learning need as drug management, within 6 months I shall do all I can to achieve proficiency in the administration of drugs. I am fully aware of the complexities of drug administration such as, the 10 R’s which I mentioned above, new medications coming on stream, old drugs being disused or superseded and contraindicated where certain combinations of medication is not advisable, the list can go on and on. As a nurse managing drugs I know there is no room for guessing when drugs are concerned, I know the only way is the right way when lives are at risk.
1
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gibbs reflective cycle"
Gibbs' Reflective Cycle was developed by Graham Gibbs in 1988 to give structure to learning from experiences. It offers a framework for examining experiences, and given its cyclic nature lends itself particularly well to repeated experiences, allowing you to learn and plan from things that either went well or didn’t go well. It covers 6 stages.
Related Articles