
INTRODUCTION
This brief considers role of the nurse in the HIV prevention and care in the black African community. The document considers empirical literature from academic, governmental, and other sources. It is argued that the available evidence is too scant to warrant conclusive inferences about the role of nurses in HIV care and management for this ethnic group. This is compounded by ambiguities about the role of nurses in promoting sexual health, and uncertainty about the appropriate criteria for evaluating their impact on the African community.
Black Africans in Britain
According to the Department of Health (2005b) approximately 480,000 people living in England (less than 1% of the population) have Sub-Saharan African heritage, by birth and /or descent. More than 75% live in the Greater London area, mostly in inner London Boroughs. Compared to the rest of the UK population, Africans tend to be younger, well educated (just 13% of Africans reported have no educational qualifications), more likely to be unemployed and living in rented (often overcrowded) accommodation. Asylum legislation has meant that a significant proportion of the population has questionable migration status in the UK. New arrivals in the UK, including asylum seekers, are offered a medical examination that may include a HIV test if this is requested, or the medical examiner judges that a test is necessary. The test result is not necessarily considered when an asylum application is processed.
Many Africans live in isolation, separated from friends and family back in Africa, (for asylum seekers), with no access to public funds, and struggling to adapt to a new culture (Millar & Murray, 1999). Many are struggling to learn English.
Sexuality is heavily influenced by traditional (tribal) beliefs, taboos, customs, religion, and spirituality. HIV is virtually a taboo subject. Thus, a sero-positive status has a significant effect on various aspects of a persons life, including problems dealing with the diagnosis, ambivalence about whether or not to test, gender issues (e.g. whether or not to breastfeed), and coming to terms with the possibility of death (e.g. implications for children, family) (Miller and Murray, 1999; Doyal & Anderson, 2005).
The prevalence of HIV infection is high in both the immigrant and British born/resident African populations. Asylum seekers and others with unsatisfactory immigration status have limited access to public funds, live in poverty, and generally avoid utilising public health services, until illness is at an advanced stage.
Black Women
There is considerable research on the plight of African women as distinct from men (e.g. Withell, 2000; Tabi & Frimpong, 2003). Much of this literature highlights aspects of their increased susceptibility, or predisposing factors or experiences. Motherhood is an extremely important goal for many African women, so that unprotected sex becomes a cultural necessity.
Doyal and Anderson (2004) document the devastating impact of HIV on the lives of African women living in Britain. Many women harbour serious concerns about the health of their offspring. There is a distinct reluctance to give birth to a sick (HIV-positive child). Many women have a ‘vague’ immigration status, whereby they may not be entitled to state benefits, have no work permit and/or rely on charities for subsistence.
The immigration issue is multidimensional. Many women live with a chronic fear of deportation, perhaps remaining in doors for days at a time, and/or refusing to open the door when the bell rings. Then there is the poor housing. Some put up with unsanitary and crumbling accommodation due to lack of funds and the awareness that housing conditions back home in Africa are much worse. Furthermore, some individuals become distressed or depressed because they are isolated from friends and family back home, and for a prolonged (and perhaps indefinite) period of time. Finally, many women may be unsure of their health care entitlements in the UK, and hence be unaware off and/or fail to utilise appropriate HIV care services.
Additionally, religious faith remains a stable and salient characteristic of Black African culture. In the face of adversity many women turn to religion for ‘hope’ and ‘deliverance’. Doyal and Anderson (2004) quote one woman: “I have turned to God. I have really got to know more about God now. I know God exists… . God is in control. I know there is an afterlife here” (p.1736). The danger is that some women may seek therapeutic remedy from God, as a substitute for seeking medical care.
Epidemiology
According to Department of Health (2005a) figures provided by the Communicable Disease Surveillance Center (CDSC), up to 12,558 black Africans living in England by 2003 were HIV-positive. This figure was based records from HIV treatment clinics and care centers in England, and accounts for 36% of the total number of people in England living with HIV. In 2003 69% of heterosexual HIV-positive people (or 2624 individuals) were probably infected in sub-Saharan Africa. The majority of cases (65%) were female. In 2002 black Africans accounted for 70% of the total number of diagnosed HIV infections. Furthermore, “of the 15,726 heterosexual men and women seen for care in England, Wales, and Northern Ireland in 2003 for whom ethnicity was reported, 70% (11068) were black African, 19% (3009) were white and 4% (657) black Caribbean. Africans feature in all the main transmission routes for HIV…” (p.12) (see Figure 1). HIV positive Africans tend to be diagnosed much later in the course of the HIV disease, and show low uptake of clinical monitoring and antiretroviral treatments.
Focus: The North West of England
The North West HIV/AIDS Monitoring Unit (2005a, 2005b), based at the Center for Public Health at Liverpool John Moores University, regularly and comprehensively
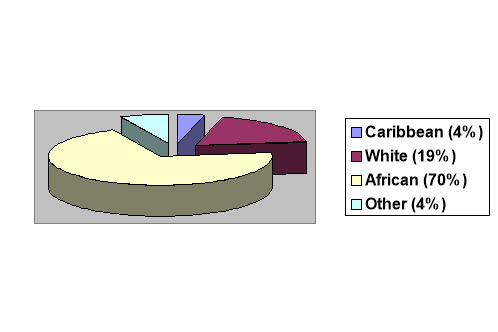
Figure 1 Distribution of HIV infections (those seen for care) across ethnic groups in 2003
monitors HIV trends in Northwest of England. The surveys are supported by the Health Protection Agency and the Northwest Public Health Observatory, and cover three main regions: Cumbria and Lancashire, Cheshire and Merseyside, and Greater Manchester. The Units data reflects both new and total HIV cases and dates back to 1996.
The total number of HIV cases virtually doubled over the nine-year period from 1996 to 2005, rising from fewer than 300 in 1996 to over 600 by mid 2005. The data suggests that black Africans living in the Northwest have an unusually highly risk of contracting HIV compared to other ethnic groups. This trend applies to both newly diagnosed HIV cases from January to December in 2004 and 2005, and total HIV cases by the end of these periods. Also, this pattern seems to echo national trends.
Africans accounted for almost a quarter (23.1%) of total HIV/AIDS cases (3574), by far the highest figure of all ethnic minority groups. For comparison, black Caribbeans made up less than one percent (0.7%, or 26 cases). The vast majority of black Africans (93.1%, or 769 of 826 cases) contracted HIV through heterosexual interactions. This contrasts sharply with Caucasian cases, of whom more than three-quarters (75.2%) contracted the virus through homosexual intercourse. When the data was collapsed by gender, again, black African women accounted for the majority (63.4%) of the 857 females diagnosed with HIV.
These findings may be confounded by significant variations in the distribution of ethnic groups across the UK and native (British born) versus immigrant status. For example, population census figures show a much higher population density for black Africans compared with black Caribbeans in the Northwest regions. This may partly account for the over representation of Africans in some categories. Furthermore, it is not clear whether patterns observed are statistically significant. On the other hand the proportion of Africans amongst new and total HIV cases is over represented when compared with the proportion of Africans in the overall UK population.
Current Health Strategies
Prior to 2001 there was no official health strategy for promoting sexual health in Britain. In July 1999 the Secretary of State for Health presented a white paper to Her Majesty, the Queen, titled Saving Lives: Our Healthier Nation (The Stationary Office, 1999). Curiously the HIV/AIDS threat received little mention in what was otherwise a comprehensive document on the Governments health policy. The lack of an elaborate national strategy for HIV/AIDS meant that the steady increases through the 1990s in HIV-related morbidity and mortality (North West HIV/AIDS Monitoring Unit, 2005a) went virtually unchecked. This all changed in 2001 when the Department of Health published the National Strategy for Sexual Health and HIV (Department of Health, 2001, 2002, 2005a, 2005b). The strategy outlines several generic aims:
- Reducing the transmission of HIV and other STIs (Sexually Transmitted Infections);
- Reducing the prevalence of undiagnosed HIV and STIs (in other words, increasing HIV testing for people at risk).
- Improve health and social care for HIV-infected people;
- Reducing the social stigma associated with sexually transmitted diseases, notably HIV.
In 2005 the Department of Health published more detailed objectives for HIV prevention specifically within the African community (Department of Health, 2005b). These objectives were as follows;
HIV Prevention:
1.Reducing transmission (sexual and vertical);
2.Reducing prevalence of undiagnosed HIV cases;
3.Eliminating the stigma associated with sero-positive status.
Health and Social Care:
1.Ensuring that HIV-positive Africans have equal access to services;
2.Ensuring that those services are culturally sensitive;
3.Ensuring that service delivery is based on assessment of individual need;
4.Facilitating access to testing;
5.Making special provision for children and adolescents;
6.Improving adherence to anti-HIV treatment regimes;
7.Creating better access to education, employment and leisure;
8.Supporting carers and families;
- Eliminating social exclusion is minimized.
Several strategies for prevention are outlined. The first plan is that HIV prevention must operate at both an individual and structural level.
Prevention activity at the individual level must address knowledge deficiencies (e.g., awareness of available health services), tackle inappropriate attitudes, beliefs, perceptions, and intentions, and teach relevant skills (e.g., condom negotiation). These goals can be achieved through various interventions including one-to-one counseling, out-reach work, telephone help lines, the internet, provision of sperm washing services, and clinical interventions to prevent mother-to-child transmission.
Structural prevention measures include reducing poverty, introducing and implementing appropriate laws and regulations, and modifying societal factors (e.g., social norms, stigma, discrimination), and organisational factors (e.g., supporting community health organisations). Structural change can be achieved through group, community, and socio-political level interventions.
Strategies for social care include: making peer support available at special ‘flashpoints’ of maximum need (such as at diagnosis, or during times of emotional distress), in order to improve adherence to treatment regimes; and providing support, advice, and education to sero-positive people, to help them to return to education.
Additionally, the Department of Health (2005a) has clarified how the National Strategy for Sexual Health can be implemented by primary medical services, through four contracting routes: Primary Medical Services (PMS), General Medical Services (GMS), Alternative Provider Medical Services (APMS), and PCT-led Medical Services (PCTMS). All four services rely heavily on nurses, and “provide flexibility and opportunities to tailor services around the needs of the patients” (p.17). Thus, in theory, the current sexual health strategy can be tailored to meet the needs of minority ethnic groups.
RATIONALE
Black Africans are the minority ethnic subgroup most at risk for contracting HIV/AIDS in the UK. It is therefore widely acknowledged that this group has special care and management requirements (Department of Health, 2005a).
Gaps in Care and Practice
This report reviews the literature on nursing HIV care provision specifically for the black African community. The review identifies various salient issues that need to be addressed:
1. Uncertainty about the role and effectiveness of nurses in prevention and care of this ethnic group.
2. Insufficient empirical evidence on various aspects of prevention/care including; the role of nurse in facilitating uptake of antenatal testing by African women, and HIV testing by Africans in general; the degree of involvement and effectiveness of nurses in community-based African HIV/AIDS projects; sensitivity to cultural factors in, palliative care, and self-management; Dealing with the HIV stigma and its effect on health service utilisation; and nurses roles in supporting involuntary care provision.
3. Inadequate evidence on the role that African nurses can play in reducing cultural barriers, and providing liaison and training services.
LITERATURE REVIEW
Literature searches were performed using several electronic data bases: PSYCHINFO (BIDS), INTERNURSE, Academic Search Premier (EBSCOhost databases), British Medical Journal On-line, HIGHWIRE Press, SOCIAL CARE Online, Department of Health database, and the Internet. Various combinations of the following key words were used: nurse, nursing, care, African, black, ethnic, minority, women, sub-Saharan Africa, community, HIV, AIDS, palliative, and antenatal[1].
Priority was given to studies published from the late 1990s, although due to the paucity of literature some earlier studies are reviewed. Furthermore, emphasis was placed on UK studies. However, limited evidence from Sub-Saharan Africa is considered to highlight certain cultural issues.
Finally, the review is structured in relation to prevention (including antenatal testing and transmission through breastfeeding), and health and social care (Department of Health, 2005a).
The Nurses Role
The National Strategy for Sexual Health and HIV (Department of Health, 2001, 2002) illuminated the rise in HIV sero-prevalence for ethnic minority groups in Britain. Nursing care was identified as essential in managing sexually transmitted diseases and promoting sexual health in these groups.
The prevention and care strategies for African communities, specified by the Department of Health (2005b), provide a framework for nurses to tailor their roles to meet the cultural needs of sero-positive Africans. Miller and Murray ((1999) provide a comprehensive account of some of these cultural characteristics, specifically regarding response to a positive diagnosis, parenting issues especially for HIV-infected mothers, problems of disclosure, attitudes towards death, immigration issues, and common health care dilemmas, and effective engagement between carer and patient.
Training
According to the Medical Foundation for AIDS and Sexual Health (2003) nurses do not receive any special training in HIV care and prevention. The Nursing and Midwifery Council (NMC) approves special HIV training courses for nurses but these are not offered in all universities and colleges, and may be optional at institutions that offer them. According to Campbell (2004, p.169), “Pre-registration training for nurses does not include mandatory education relating to sexual health services. Nurses working in sexual health gain post-basic education in an ad-hoc manner – through working in the specialty, and by undertaking specialist post-registration courses”. Moreover, although the NMC regularly monitors courses, it does not scrutinise individual courses that confer no special qualification, so that they may be considerable variability in the quality of courses offered in different institutions.
Thus, it is possible that a large percentage of nurses have no special knowledge or skills in HIV prevention/care for ethnic minority groups. It follows that many nurses that may be ill prepared to deal with the particular HIV needs of African communities. However, nurses who work in Greater London, and hence are regularly exposed to African patients/communities, may quickly acquire some degree of ad-hoc expertise. By contrast nurses based in other parts of the country with smaller African communities may be especially uninformed and inexperienced.
Role Ambiguity
In the absence of mandatory HIV training, there may be some ambiguity about the precise roles/tasks nurses are required to perform in HIV care/prevention. Campbell (2004) notes that career pathways are patchy and ill defined, and it may be necessary for nurses to undertake placements in key areas of sexual health. Certain aspects of HIV care are applicable to other diseases, and hence may form part of a nurse’s standard training and job description (e.g. antenatal testing, patient pre-admission assessments). However, certain tasks are specific to HIV and/or a particular population group. Some nurses may be uncertain whether such roles are within their jurisdiction. For example, whose job is it to reduce the powerful HIV stigma that prevents many sero-positive Africans from testing for HIV, and/or benefiting from family support? Who is responsible for addressing cultural taboos and totems?
Palliative Care
This refers to nursing care aimed at maximising the quality of life for terminally ill patients, for example by reducing pain and discomfort. The National Council for Hospice and Specialist Palliative Care Services (NCH-SPCS) identifies seven domains of palliative care: increasing patient/carer understanding of diagnosis/prognosis; alleviating pain/symptoms; facilitating patient independence; reducing patients/carers negative affect (e.g. anxiety, depression); soliciting support from other agencies; advising on appropriate care locations as illness progresses; supporting families/carers, before/after death.
To what extent do nurses meet these requirements met in sero-positive black African patients?
There is a paucity of research addressing the palliative care needs of black African patients specifically. However, some studies have examined the needs of ethnic minority groups in general (Jack et al, 2001; Diver et al, 2003). Various barriers to effective palliative care for ethnic minorities have been identified including communication difficulties and the lack of trained interpreters (Jack et al, 2001).
Diver et al (2003) conducted a qualitative study to identify the specific palliative needs of ethnic minority patients attending a groups regarding palliative care. Participants comprised two Jamaicans, one Indian, and one from the Ukraine, but no black Africans, who attended the day-care center once or twice weekly, for up to a year. Several key themes emerged. One concerned the individual needs of the patients, which were not related specifically related to culture (e.g. diet, religion, day care, avoiding social isolation). Two other themes highlighted attempts to fit in with the dominant culture, for example by eating English foods and communicating with staff in English. Another theme highlighted positive perceptions of palliative care: participants expressed gratitude to staff, with one individual noting “the Macmillan nurse had been sympathetic and had not pressurised her when she decided to stop having chemotherapy” (p.395). However, participants reported that staff had not inquired about their culture albeit they simultaneously felt their cultural needs were being addressed. Although Diver et al’s (2003) study involved a very small sample, the findings suggest that nursing staff can effectively meet the palliative needs of minority patients.
Some evidence suggests that nursing care can be more effective when a liaison professional is involved. Jack et al (2001) assessed the value of a ‘liaison’ worker that mediates between ethnic minority patients, their families, and health care staff. This study focused on the role of an ethnic minorities ‘liaison’ officer, appointed in May 2000. The workers brief is to facilitate palliative care amongst the Asian community specifically. Thus, he/she helps with communication, religious, gender-specific, bereavement, and other issues. However, several case studies are presented that illustrate the difficulties inherent in using a liaison person. For example, the liaison role is emotionally demanding and health care staff sometimes assume the liaison worker has medical expertise. Nevertheless, the concept of a liaison worker may improve the job performance of nursing staff involved in palliative care.
Hill and Penso (1995) make recommendations that tailor palliative care to the needs of ethnic minority groups. These include: ethnic monitoring; having an equal opportunity policy; enforcing a code of conduct; staff recruitment/training; developing a communication strategy; health promotion; facilitating culture-specific care provision; appropriate food policies; community health initiatives. Given the paucity of research evidence focusing of HIV-positive black African patients in the UK, it remains unclear the extent to which these strategies facilitate effective palliative care in this population group.
Some evidence is available concerning palliative care delivery in sero-positive women living in Sub-Saharan Africa (Defilippi, 2000; Gwyther, 2005). This evidence may provide additional insights that may apply to the care of black Africans who have emigrated to the UK. Gwyther (2005) documents the nature of palliative care in South Africa. Here, hospice care is primarily performed at home, with only a few inpatient units available on a short-term basis to selected patients (e.g. those with serve symptom control problems). A comprehensive ‘community-based home care programme’ has been established, in which patient care is provided by the local community (e.g. extended family, neighbours), but managed by health care (hospice) staff. Thus, “there has been a shift away from the conventional hospice domiciliary nurse as the primary caregiver to community care workers, who are trained, supervised, and supported by the professional nurse” (p.113).
This South African model has several advantages when applied to the UK theatre: Firstly, training extended family members (and perhaps even neighbours) in palliative care, with the aim of managing AIDS, and decreasing transmission of the HIV virus, may help resolve problems of communication, diet, custom, and other culture-specific issues that the patient considers relevant. This model goes some way to address Hill and Penso’s (1995) recommendations for recruitment/training, effective communication, culture-specific care, suitable food policies, and community health initiatives. The professional nurse, free from some primary responsibilities of care, may be able to commit more resources to ethnic monitoring, enforcing codes of conduct, and ensuring equal opportunities in practice.
Evidence-Based Practice
There is a growing requirement in nursing and (other medical specialties) for evidence-based medicine/decision making (Thompson, et al, 2004). Evidence-based practice is particularly essential in the care of minority groups due to the relatively greater level of cultural ignorance in health care about ethnic minority customs compared with the dominant culture (Serrant-Green, 2004).
There is a paucity of research assessing the degree to which nurses refer to empirical evidence when making clinical decisions about black African HIV patients. Thompson et al (2004) suggest that, in reality, nurses rarely consult evidence when making clinical decisions, irrespective of the patients’ background. Instead they are much more likely to consult their colleagues for information for advice. This is worrying because clinical decisions can be made about black-African patients based on incorrect assumptions rather than fact. For example, Gibb et al (1998) highlight the possibility that nurse midwifes may fail to offer antenatal HIV-testing to black African women, for fear of appearing discriminatory. Yet, there is little or no evidence about how black women may actually perceive such offers.
Overall, there is a paucity of research on the role and effectiveness of nurses in delivering health and social care to the African community. Studies that focus on “black” patients (i.e. Afro-Caribbean or African parentage) cannot be generalised to Sub-Saharan Africans as HIV/AIDS incidence and prevalence is significantly different for these groups, suggesting different health care requirements. Similarly, data collected from Asians, Bangladeshis and other UK minority groups is generally inapplicable as the cultures are vastly different.
The role of African Nurses
A significant number of black African nurses work for the NHS. These individuals may play an important role in facilitating HIV prevention and care in the African community (Andalo, 2004; UNISON, 2005). There are two ways this may happen. Firstly, African nurses can serve as ‘in-house’ liaison workers, improving communication and eliminating cultural barriers between the health service and African communities. Secondly, African nurses can help in ‘educating’ other health-professionals on fundamental cultural issues, both in relation to the African community as whole, and individual sero-positive patients.
The Department of Health (2000b) acknowledges the significant contributions of African nurses to sexual (and other) health issues in the African community, in the form of the Mary Seacole Leadership Awards. A recent article published by BioMedCentral (Batata, 2005) indicates that over 3000 nurses trained in Sub-Saharan Africa were registered to work in the UK in 2002/2003. These nurses originated from eight countries (South Africa, Nigeria, Zimbabwe, Kenya, Zambia, Malawi, Botwana and Mauritius), most of which have high HIV sero-positive prevalence rates. It therefore follows that these professionals will be very familiar with HIV preventive and care measures that work effectively with African communities.
Approximately a quarter of all the foreign trained nurses registered during 2002/2003 (i.e. including nurses from non-African countries) worked in or near London, with 49% based in other parts of England, suggesting that there is a significant nurse pool available to support African communities in the London area. Unfortunately, there is a lack of research evidence on the role of African nurses in facilitating HIV care and prevention in African communities.
Most studies focus on immigration, recruitment, or discrimination issues, rather than job performance and impact on care provision for local communities. The World Health Organisation (2003) indicates that one of the three top non-EU source countries for international nurses working in the NHS is from a Sub-Saharan African country (South Africa). The number of nurses recruited from Zimbabwe has increased recently. Nevertheless, recruitment and retention remain a problem. Although the NHS is thought to have one of the most effective nurse recruitment schemes in the public sector, there are still problems recruiting African nurses. For example, Andalo (2004, p.17) notes that although there has a been a significant increase in the number of Africans applying for nurse diploma courses, the rejection rate was more than fifty percent higher for African compared with white applicants. However, an argument for more recruitment can be better formulated given empirical evidence on the value of African nurses in promoting HIV prevention and care in their community.
Department of Health (2005b) highlights the “need for basic information regarding HIV transmission, testing, and treatment. In particular, cultural practices that place some Africans at particular risk of transmitting or acquiring HIV requires specific, culturally competent attention” (p.13). Community nurses play an important role in this regard (Hoskins, 2000). Moreover, effective dissemination of knowledge requires collaborations between health professionals and agencies, access to services, and other recommended measures (Department of Health, 2000a, 2001, 2002, 2005a, 2005b).
Community Nursing
Community nursing care for sero-positive Africans in Britain has expanded rapidly over the last decade, reflecting a national shift in emphasis towards community care (McGarry, 2004). The Department of Health framework for prevention and care emphasised the importance of partnerships between HIV prevention agencies, Primary Care Trusts, local African community-based organisations, and other establishments (Department of Health, 2005b).
According to the Department of Health (2005b), over 75% of black Africans in Britain live within Greater London. The largest concentrations live in Inner London Boroughs, which also have high sero-prevalence rates. Thus, the role of community nursing in the Greater London area is of particular interest.
There is some evidence of collaboration between different agencies. One south London HIV partnership incorporates up to fourteen HIV prevention organisations, including several African-based projects: One African project covers up to nine catchment areas (Croydon, Kingston, Lambeth, Lewisham, Merton, Richmond, Southwark, Sutton, Wandsworth), and promotes the access to and utilisation of local HIV care and support services. This project recently launched a new treatment service designed to encourage men to adhere to treatment regimens.
There is a paucity of research on the efficacy of such partnerships in reducing the spread of HIV in the black African Community.
More importantly, there is limited empirical evidence on the involvement and impact of community nurses in these projects.
The partnership in south London offers complementary HIV care services across the local area. Some of these services are available from local HIV clinics, were nursing staff presumably play a key role. Furthermore, there appears to be specific community nursing provision for children and families. For example a children’s hospital in Croydon offers nursing care for HIV-infected children and their families. Community nursing services are also available for adults.
A study was commissioned to review progress on African HIV prevention initiatives in Enfield and Haringey, from 1997 to 2002. The investigation collected data on HIV-prevention needs, and voluntary and statutory sector provision, all of which are implemented by nurses (e.g. health visitors, community nurses, nurse midwifes).
It was found that a lay referral system, operated solely by friends and family, worked effectively. Medical support from nurses and other health professionals was requested when symptoms become too serious. Compared with other ethnic groups HIV-positive Africans were more reluctant to test for HIV, and those who were sero-positive showed lower uptake of anti-retroviral treatments. Furthermore, there was evidence of poor attendance at clinical monitoring sessions, and it was argued that lat
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "HIV"
The human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) pandemic is one of the most serious contemporary sexual health related issue affecting the human race today. By the end of 2009, it was approximated that 34 million people were living with the HIV virus and deaths related to AIDS were about 1.8 million people.
Related Articles
