This case study discusses podiatric management of a patient presented to a podiatry clinic with heel pain, upon referral from a General Practitioner. A brief description of the patient’s condition, the aetiology of heel pain, patient assessment leading to possible diagnosis and deferential diagnosis will be outlined. This is followed by discussion on the short, medium and long term podiatry management. Patients’ education and the psychosocial factors influencing the management as well as the outcome measures of intervention will also be discussed.
The patient in this case study is referred to as Emily blunt (Emily). Emily is 36 years old and works as a woman police constable (WPC). Emily complains of a sore foot which started a few weeks ago. Emily explains that the pains appear worse in the evening, but there is a pain of stiffness which is very hard to manage first thing in the morning. She manages the pain with Solpadine which she buys over the counter. Emily recently joined the local gym in an effort to help regulate her weight and to improve her fitness. Emily looks after her mother’s dog which she takes for a walk. Emily asserts that palpation of the heel around both lateral and medial ankle area elicits pain as well as pressing of a thumb around the anteromedial aspect of the calcaneal.
Heel pain is a very common foot problem usually encountered by podiatrist (Navrvaez et al., 2000). According to Bergmann (1980) the origin of heel pain is multi-factorial. It is usually not caused by a single injury, such as a twist or fall, but rather the result of repetitive stress and pounding of the heel ( Woelffer et al, 2000 ) which usually presents in the form of pain either under the heel or just behind the heel, where the Achilles tendon connects to the heel bone (Brown, 1996). In most cases the pain is under the foot towards the front of the heel (Schuberth, 1990)
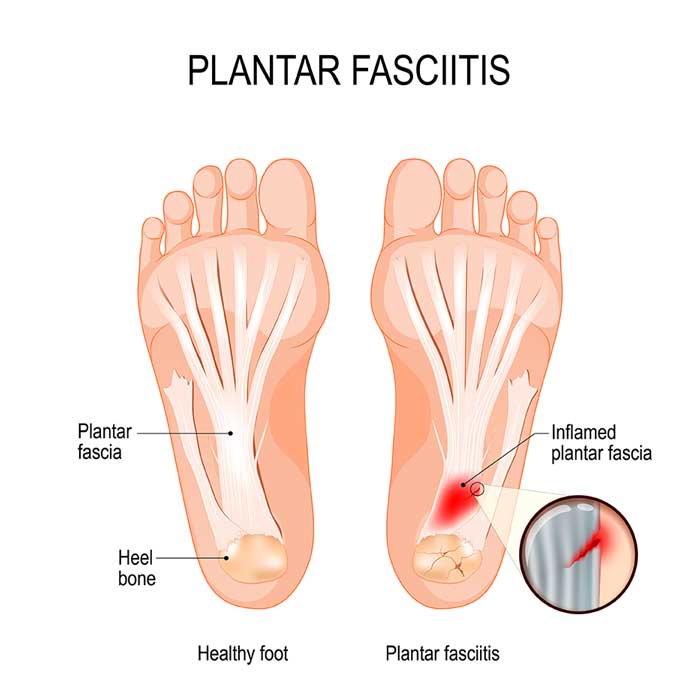
Current literature regarding heel pain, suggest Plantar Fasciitis (PF), inflammation of the plantar fascia as the main cause. Most cases of plantar fasciitis are the result of a biomechanical defect that causes abnormal pronation (Martin et al, 2001). For example, a patient with a flexible rearfoot varus may at first appear to have a normal foot structure but, on weight-bearing, may display significant pronation. The talus will plantar flex and adduct as the patient stands, while the calcaneus everts. This pronation significantly increases tension on the plantar fascia. Ankle equinus, rearfoot varus, forefoot varus, and limb length variation, can also lead to an abnormal pronation and cause additional stress on the origin of the plantar fascia (De Garceau et al, 2003).
As in the case of Emily, many people who experience PF describe it as pain in the heel with their first steps in the morning, after getting out of bed. It feels like a sharp stabbing pain at the bottom or front of the heel bone (Balint, 2003). According to Kosinski and Lilja (1999), the pain, in most cases is more severe following periods of inactivity, like early in the morning or after sitting for a long period. After walking around for a while the sharp pain subsides and it is replaced by a dull ache (Kosinski and Lilja (1999). However, the symptoms may become worse again getting to the end of the day (Balint, 2003) as seen in Emily’s case. Other common causes of heel pain include Calcaneal Stress Fracture which has symptoms that closely resemble those usually associated with PF, Nerve Entrapment, Siastica, Heel bursitis, Tarsal Tunnel Syndrome, and some systemic condition such as Systemic lupus erythematosus (Lemont, Ammirati and Usen, 2003).
The podiatrist may diagnose planter fasciitis based on the patient’s detailed medical history and the clinical presentation. In Emily’s case, the podiatrist will undertake a thorough physical examination which will include musculoskeletal and biomechanical assessment and ask pertinent questions about the pain. The podiatrist may ask the patient whether their daily activities involve walking and standing excessively; which Emily does. Emily’s physical examination should include inspection of both feet at closed and open chain to look for any abnormal pronation or other biomechanical irregularities. The podiatrist may palpate bony prominences especially over the medial calcaneal tubicle, noting any tenderness or palpable defects. This will elicit pain which is generally local at the origin of the anatomical central band of the planter fascia, with no significant pain on compression of the calcaneus from the medial to lateral direction. Palpating the medial band of the planter fascia while passively dorsiflexing the toes and thereby activating the windlass mechanism can also cause discomfort. It is important to note patient’s foot type as well as quality of footwear. Gait analysis can be done by the podiatrist observing the foot while Emily is walking, this may help identify gait abnormalities. Passive range of motion of the foot and ankle should be assessed for indications of restricted movement. Any discrepancies in limb length should also be noted. During the physical examination, it is also important to assess for any neurological changes and check for any nerve irritations (Tinel or valleix sign) .While imaging is not often used in the diagnosis of plantar fasciitis; they may be requested in order to narrow down differential diagnosis like calcaneal stress fracture.
After diagnosing a patient with plantar fasciitis, the treatment is a two-step process (Landorf et al, 2004). The first step outcome is to decrease the patient’s pain level by at least 90 percent. Conservative treatment are icing, stretching exercises, rest and activity modification, shoe inset and non-steroidal anti-inflammatory drugs (NSAIDs) (Thomas et al, 2010).
Emily is quite young, active and has recently got herself into more activities such as going to the gym and walking her mother’s dog. She also plans to support her partner in the marathon. Therefore Podiatry treatment goal for Emily will be reduction of pain and inflammation.
Ice can be applied via ice massage or ice pack onto the facia. Crushed ice can be placed in a plastic bag wrapped in a towel, then applied for 15-20 minutes (Young, Rutherford and Niedfeldt, 2001); the use of crushed ice allows the pack to be moulded to the foot, thereby increasing the contact area. (Alfredson and Lorentzon, 2000).
Rest and activity modification (Reid, 1992) is vital to the treatment of plantar fasciitis. Complete rest may not be practical for more active individuals like Emily considering the nature of her job. Alternatively, Emily must alter activities that can exacerbate the pain. A dieticians help will also be invaluable if Emily is to check her weight.
Research has shown manual stretching to be ineffective, because patients do not stretch correctly and consistently (Kleisinger, 2003). Since equinus and tight gastrocnemus and soleous is often one of the aetiologies of PF, it is important to address this issue for pain reduction and prevention of recurrence. Wall stretching for at least 15 to 30 minutes daily (REF) will be effective for Emily, under the supervision of a physiotherapist.
Emily may be given an insole with a valgus filler padding. The padding could be manufactured from a semi-compressed foam. The thickness will depend on the severity of the pronation and the patient’s foot wear. The edges should be bevelled for comfort and to guard against any secondary problem.
Several classes of drugs have a role to play in musculoskeletal injury management. But their use should be closely monitored because of the risk of dependence and abuse (Gill and Kiebzak, 1996). Non-steroidal anti-inflammatory drugs (NSAIDs) like short-acting indomethacin or diclofenac taken orally could be prescribed by Emily’s GP. These provide a combination of analgesic and anti-inflammatory effects and are particularly useful in conditions with ongoing inflammation (BNF, 2007) as in Emily’s case.
Many patients attempt self remedies before seeking medical advice. Emily is concerned because she has been on a self medicated Solpadine. Solpadine contains codeine, caffeine and paracetamol; paracetamol overdose may cause irreversible liver damage and bleeding. Caffeine causes nervousness and gastro intestinal disturbances and codeine, drowsiness. Prolonged use as in the case of Emily may lead to addiction and result in withdrawal symptoms once the drug is stopped (BNF, 2007) and Emily may need counselling in other to cope.
PF is a self-limited condition. Studies have shown that it lasts for approximately 6 to 12 months. The podiatrist will expect to see Emily in 6 months time with an improvement in pain, acceptable weight and a considerable level of exercise tolerance.
If Emily’s symptoms are not improving, then the medium term management plan would be steroid injection. Steroid injections are well documented for the treatment of PF, but must be used with caution in other not to cause other damages to the fascia (Tsai, Wang and Tang, 2003). The long term goal for Emily will be to correct any biomechanical defect and to prevent reoccurrence. This can be achieved by using customized orthoses and a more invasive surgical treatment. (Lee, McKeon and Hertel, 2009).
Patients may respond to an injury and pain with mood disturbances, including depression, lowered self esteem, anxiety, anger and maladaptive behaviour (Braddeley, 1990). Although Emily appears strong and motivated, accepting the change in lifestyle will be with difficulty. Her inability to train as she would have wanted, in order to achieve her plan to support her partner and the difficulty she has to endure when it comes to walking the dog will make her worry. In this case, patient education to address psychosocial issues that may militate against Emily’s progress is very vital for better treatment outcomes (Lazarus and Folkman, 1984). Calm explanation, reassurance and involving her in deciding the management plan can help work against these psychological disturbances. Education and supportive counselling; giving literature explaining the condition are also good (Kaplan, 1986). Also, structures within her work place should allow her to take a break or work minimal hours while she recuperates. If there is the need, a referral to a psychologist for counselling would also be helpful. Understanding the stresses in Emily’s life and finding ways to help her cope could lead to better patient engagement for treatment success.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "plantar fasciitis"
Plantar fasciitis is one of the most common causes of heel pain. It involves inflammation of a thick band of tissue that runs across the bottom of your foot and connects your heel bone to your toes (plantar fascia). PF is usually diagnosed and common with runners, but can also be related to those that are obese.
Related Articles