Hypoxia – caused by airway obstruction; respiratory distress or failure or sepsis. Achieve a safe and secure airway, this can be achieved by head/tilt chin lift manoeuvre – Head injury patients should be jaw thrust. Ensure the airway is clear, suctioning may be required used a sterile yankeur to remove secretions, vomit or blood. High flow oxygen should be prescribed and administered using a non-rebreather mask (trauma mask), 15litres of oxygen and delivering 85-90% Oxygen. Intubation may be required using an endotracheal tube and bag-valve mask (using 2 people) – good bilateral air entry should be observed to check positioning of ET Tubing.
Hypovolaemia – caused by haemorrhage such as a ruptured aortic aneurysm; trauma; sepsis; gastrointestinal bleed or burns. 2 large wide bore peripheral cannula (14-16g) should be inserted using an aseptic technique and trained professional. Fluid resuscitation should be commenced to improve intravascular volumes and therefore attempting to maintain or improve blood pressure. Crossmatch should be obtained for transfusion. O-Negative blood supplies can be used whilst waiting for blood component to arrive. Immediate surgical referral will be required in an attempt to arrest bleeding.
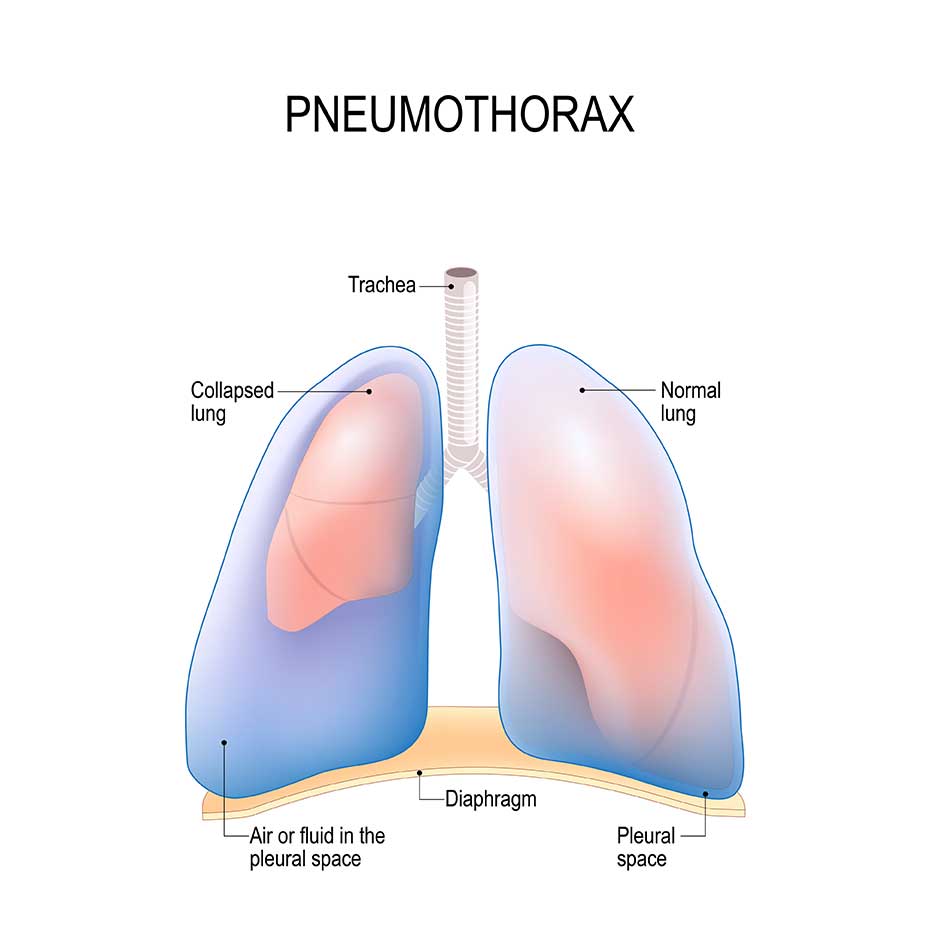
Tension pneumothorax – caused by chest trauma, ie a fractured rib, asthma, Central venous pressure line incorrectly inserted, all of which can damage the integrity of the pleural membranes (parietal and viscerial) allowing air into the pleural space causing the lung to collapse. There may be signs of a tracheal deviation. A large bore cannula should be inserted into the mid-clavicular line; and a chest drain used and inserted into the second intercostal space. This draws out the air within the pleural space into the drainage system.
Toxic/therapeutic disorders – caused by drug overdose or exposure to toxic substances within a work capacity. All members of staff should be well protected and appropriate clothing worn so that there is no cross-contamination of toxic substances. If the toxin substance can be identified then staff can con consult ‘toxbase’ to understand more about the substance and identify a suitable antidote. In overdose, a blood sample can be taken and sent to biochemistry to identify the levels of toxicity to then aid decision to the amount of antidote required.
364 words
Part A Question 3
Eyes Opening
Eyes open to speech – on the Glasgow Coma Scale 3 (eyes opening). Eyes opening indicates how well that patient can be aroused called the ‘arousal mechanism’. If Ian’s eyes were closed when the nurse approached him then verbal stimulus should have been used for example the nurse may have called the patient’s name in a normal tone voice. At this point Ian would have opened his eyes. If the patient was is a deep sleep then a louder tone of voice should have been used, perhaps in both ears as he may have a hearing impairment. On baseline recording Ian’s eyes opened spontaneously, this may have been when the nurse approached him alerted by his subconscious and sensing presence or they were already open.
Verbal Response
Confused – on the Glasgow Coma Scale 4. This reflects on the patients awareness to themselves, their surroundings and environment, identifying how well the nurses’ speech is understood and how well the patient can articulate, testing how well the brain processes information in the cerebral cortex. The nurse should have asked questions that relate to time, place and person and it is important to never ask the date however, the month and year can be asked. Ian has been confused in answering questions, there has been deterioration in his level of consciousness from initial baseline observation. The patient may also appear confused to where he was, and may not recognise relatives.
This should not be confused with replying to questions inappropriately or only able to communicate partial sentences as this would be Verbal response 3.
Motor Response
This assesses Ian’s ability to follow commands, using his best arm response. In Glasgow Coma Scale Assessment, motor response should be the assessment of upper body movement and legs should not be used.
The nurse may have asked the patient to lift his arms to touch his nose, or stick his tongue out. If the patient successfully followed command then he would score 6
Ian scored 5 for motor response so he therefore was unable to follow commands.
The nurse would than have applied painful stimuli to above the chin level, either supraorbital pressure or trapezium squeeze. For patient’s with facial injuries the supraorbital stimuli is not recommended. A score of 6 would indicate that Ian localised to that area by lifting his hand up to above chin level.
A deterioration scoring of 1 in the motor response or 2 overall are significant changes to Iain’s level of conciousness and should be reported. Ian as dropped by a score of 3 to 12 so I would definitely summon senior help. I would probably want to know if the same nurse has done all three assessments to ensure that the interpretation has been consistently measured. I would also want to know what the score was during the 2nd set of neurological observations and at what time they were recorded and if there was any deterioration, did anyone act upon this altered level of conciousness. Also the Glasgow Coma Scale should be undertaken alongside a ABCDE approach (recommended by the Resuscitation Council ,UK 2010) to assessment as there are a number of factors that could influence the patients level of conciousness such as cerebral hypoperfusion, hypoxia or hypo/hyperglycaemia. Respiratory changes should be carefully monitored as this is one of the first signs of deterioration in a critically ill patient. Pupil response should also take place alongside the neuorolgical assessment to establish they are both equal and reacting to light. Fixated pupils or having a sluggish reaction to light may indicate raised intracranial pressure compressing on the III Cravial Nerve called the occulomotor nerve, potentially as a result of herniation through the tentorium space.
611 words
Part A Question 5
1. It should be decided within the multidisciplinary team (MDT) who is going to deliver the bad news. Ideally it should be a member the multidisciplinary team (MDT) that knows the patient and family members, although this is not always possible. The setting should be selected, ie, a room that is clean, tidy, has tissue and a telephone and that no-one is planning to use. The nurse should ensure that there is enough chairs for all of the family and that the room is a good size for them to all be accommodated. It is important for the nurse to be able to sit down with the family members so that good eye contact can be made and it doesn’t come across that you are in a rush or hurry. Introduce yourself and let them know that you are a staff nurse and have been looking after Mrs Jones. Generally letting them know that you are there and that you carry an open and honest approach to your body language. Show them into the room and make you that on ‘occupied’ sign is placed outside the door so that there are no disturbances. Predict the information that you will require and be prepared. Know what is exactly happening with the patient and what the expected interventions and management may be. It is important to have an understanding of what has already been discussed with the family during previous communication.
2. Establish what is already known to the family about the patient. What is their understanding of the condition. They may already be aware that there risk of a further stroke occurring after the first. It may be that nurse has to start of from the beginning from when the patient was admitted. By establishing this information there is reduced risk of the nurse repeating information and an appropriate level can be understood and the delivery can be taken from that point. Understanding of level of communication can also be understood by listening to the family and the nurses communication strategies my need to be adapted to suit there communication needs.
3. The family members may have certain coping strategies in receiving bad news. It may be a protection mechanism ie from children or vulnerable family members that may find it very difficult in receiving the news. Is it therefore very important to ask the family first if they all wish to hear what you are about to deliver. They can then at that point make the decision for some people to get a coffee for example or wait outside. The nurse can direct then to a another area if they wish.
4. All the important information should be provided and delivered in such a way that it is broken down in small part so that your words can be ingested. It is important for the nurse to emphasise that they can ask questions at any time and if they what you to repeat anything then they should just ask. The nurse should continually make eye contact and observe their facial expressions as this may give away clues as to their understanding of the information you are providing. It may be that the nurse then feels that her delivery strategy needs to be adopted and that the information perhaps needs to be explained differently. Breaking up the information gives the family time to ask a questions relating to what you have just said. If you don’t know the answer then just say you’re not sure but you will find out the answer for them after everything has been discussed.
5. Continually assess their emotions, you may be able to sense it from them, from their eyes and facial expressions. Acknowledge and reactions and if your are not sure of the reaction they are experiencing then ask them. Express to them that you wish the news could be better, be empathetic and sensitive to their emotions. If they begin to speak, stop and allow them to talk, don’t interrupt and finish sentences for them, allow then time to talk. You may ask them if they wish for you to leave them for a moment, it may be appropriate to offer them refreshments, such as tea of coffee.
6. If you do leave them, then make sure they know your name and that if they wish to ask any more questions then they can ask for you, give them telephone numbers for the ward and if you are not going to be there over the following day or more. Inform them and provide them with another contact name who can help them if they wish to ask any more questions. Make sure that you speak to the other member of staff first and discuss what has been said so that she/he understands what has been discussed. Let them know that they can stay in the room as long as they wish. Explain to them that you can come and get the them when Mrs Jones comes back from the scan. Ask them if they would like you ask any more questions. Inform them of what is exactly happened now and let them know that you will keep them informed or any decisions that will be made in the future.
878 words
Part B – Ectopic Pregnancy – Question 1a
Approach Molly and give her reassurance throughout. A ruptured ectopic pregnancy is a medical emergency requiring emergency surgical intervention to arrest the internal bleeding. Healthcare professionals need to stabilise her condition using a systematic approach prioritising her care and preventing the development of hypovolaemic shock caused by low blood volume.
Psychological care of the patient and family is also a vital component to her care. Anxiety management is key to the treatment of the patient in shock and there is a direct link between anxiety and the initiation of stress response and sympathetic nervous stimulation. Anxiety in Molly’s case may be due to pregnancy loss. Information regarding, Molly’s condition and any interventions should be provided, and an open, honest and supportive relationship developed between the nurse, patient and patient’s loved ones (Bacidore V et al 2009)
Ensure her privacy and dignity is maintained throughout. Bacidore et al (2009) provide a holistic collaborative framework for dealing with pregnancy loss in the Emergency Department. They suggest that by reducing anxiety levels in the emergency department can reduce the risk of the patient developing anxiety and depression, or post-traumatic stress in her recovery stages.
Close monitoring of vital signs are necessary. The frequency of monitoring the vital signs will depend on the stability of the patient, with continuous monitoring being instigated for a patient at risk of rapid deterioration. The nurse must be aware of when observations are abnormal for the individual patient, and who to call for assistance. This might be helped by the use of early warning trigger scores. A prompt systematic approach to assessment using the ABCDE approach as suggested by the Resuscitation Council (UK) 2010.
Airway –
By talking to Molly, her airway can be assessed. If the patient is talking, then you know the airway is patent and Molly is maintaining her own airway. During this time the nurse can check if she has any allergies to medications, any medications that she is taking on a regular basis, part medications that she Is talking, last meal and drink and event leading up to her presentation. This can be incorporated into the WHO (2009) pre-operative check-list.
Breathing –
can be assessed by recording respiration – rhythm rate, depth, skin colour and the use of accessory muscles. This will indicate respiratory distress. Cyanosis would be a late sign of poor oxygenation. The respirations are one of the first signs of deterioration in the critically ill patient and should be carefully assessed. Normal respirations are 16-18 breaths per minute. A tachypneoa >20breaths per minute, may be a clinical feature resulting from reduced oxygenation and sympathetic nervous stimulation. Pulse oximerty should be carefully be used to assess oxygen saturation of haemoglobin molecules. This only monitors the circulation volume saturation and will not incorporate blood lost in haemorrhage (Higginson & Jones 2009).
High-flow oxygen therapy should be indicated to maximise the amount of oxygen being carried in the haemoglobin molecules. This is to minimise tissue hypoxia and maximise perfusion. A Non-rebreather mask or trauma mask should be used to administer 80-95% oxygen on 15 litres (Crouch 2009).
Circulation –
Molly is bleeding internally with loss of intravascular volume which reduced the venous return and therefore reducing cardiac output. Normal blood pressure can range between 110/65 and 140/90mmHg. Molly’s blood pressure is on the lower side of these normal parameters. It is important for nurses to be aware that pregnant patients have increased physiological reserves and increased circulation blood volume, and therefore have a better capacity to accommodate blood loss without compensating changes in their vital signs. Therefore, they may not show signs of shock until late in their presentation (Jones, Higginson, & Santos, 2010.
The peripheral pulse may feel weak and thready, despite being rapid. This is a result of reduced stroke volume and reduced venous return. The heart rate will increase as a result of sympathetic stimulation giving rise to tachycardia with beats over 90 per minute.
It is important to achieve access promptly before peripheral vasoconstriction takes place. Two large bore cannulae should be inserted (12-14g) and intravenous fluid resuscitation should be commenced.
Hypovloaemic shock, arises from reduced intravascular volumes. It is therefore vital for plasma expanders to be used to stabilise the intravascular volumes and therefore pressure (Garretson & Malberti 2007).
Crystalloids such as sodium chloride (normal saline) 0.9%, Hartmann’s should be used initially as they are relatively cheaper and more readily available then Colloids. In hypovolaemic shock large amount may be required and on administration, blood pressure should be monitored to assess if the fluid challenge is having significant improvement to the patient’s blood pressure.
In severe haemorrhage should be the provision of blood transfusion. Colloidal fluids should ideally be the first choice as it is readily available compared with blood components. They provide intravascular fluid replacement due to its osmolarity and therefore are able to retain water in the blood, increasing plasma volumes and stabilising blood pressure. However in albumin based colloids, there runs risk of the patient developing anaphlaxis and therefore should be considered by a senior member of staff.
Full blood count, cross-match for transfusion and urea and electrolytes (for renal function) should be taken. Informed consent should be established regarding blood transfusion. The patient has the right to refuse and alternative treatments should be explored. The patient’s identity must be confirmed – when the blood sample is taken, blood component is being collected from the transfusion laboratory , or blood fridge, and when the blood component is given to the patient. Prior to collection or requestion delivery of a blood component, nurses must ensure that the patient has a patent cannula, written and signed prescription, all the necessary equipment and that the patient is ready and prepared (Oldham, Sinclair, & Hendry 2009) The most important stage of the transfusion process is the right patient received the right blood (Oldham, Sinclair and Hendry 2009) failure to provide the right can result in devastating consequences and sever adverse reactions.
The patient may be as well as internal haemorrhage be experiencing vaginal bleeding. Dignity and privacy must be ensured and checked. If there are any signs of vaginal bleeding, pads can be used to soak up the blood and this can be used to monitor the volumes of blood lost. Continuous cardiac monitoring should be used to assess the condition of heart and to detect any changes in rhythm that may result from reduced myocardial perfusion, reduced venous return or electrolyte imbalances such a hyperkalaemia.
Disability –
assessing neurological function by talking throughout levels of conciousness can be assessed by using Alert, Verbal, Pain Unresponsive and if the patient is responding without confusion or agitation then this can be recorded as Alert. However, any signs of confusion, drowsiness, agitation should be assessed by using the Glasgow Coma Scale proving an accurate assessment of Central Nervous System levels of conciousness.
Blood Glucose levels should be monitored. A stress response may stimulate excessive blood glucose resulting in hyperglycaemia – this can be managed by the use of prescribed insulin, a syringe driver may be required to stabilise blood glucose levels (McLeod 2004) .
A gynaecological consultant/surgeon will be required and a pre-operative check-list completed. Informed consent should be obtained – key guidelines are located in WHO (2009)
1184 words
Part B – Ectopic Pregnancy – Question 1b
Stage 1 – Infection
In relation to the scenario, the source of infection may be: Surgical Site Infection (SSI);
Chest Infection/pneumonia (resulting from post-operative complication; Urinary Tract Infection (Urinary Catheter); Cannula Site Infection (NHS Evidence 2009)
The SSI may show the cardinal signs of infection:
Redness (erythema); Swelling (oedema); Heat; Pain; Pus/Purulence/Discharge
The redness may be centre of the wound and there may be signs of it travelling from the wound site. Swelling and oedema is part of the normal inflammatory response to infection. Heat is due to the increased metabolic activity resulting from the inflammatory response. Pain, this may be sudden pain and can may be localised to the site of infection(wound site) (Santy 2008).
UTI may be detected by offensive smelling, cloudy urine, urinalysis results with indicate leukocytes and nitrites (Creed & Spiers 2010).
Chest Infection as a post surgical complication – the patient may have a productive cough producing green coloured sputum.
SIRS – Systemic Inflammatory Response Syndrome.
Diagnostic Criteria –
Body Temperature >38 degrees Celsius or
Respiratory Rate >20 breaths per minute
Heart Rate > 90 beats per minute
White Cell Count 12×10 to the power of 9/L
(NHS Evidence 2009)
Stage 2 – Sepsis (Hyperdynamic Stage)
Sepsis can be the presumed or confirmed infection plus two or more of the above diagnostic criteria.
In early stages of sepsis, the infection and inflammatory response is now systemic and no longer local to the site of infection.
The patient may express that they feel unwell (malaise) (Steen, 2009)
Widespread oedema resulting from leakiness from intravascular space which results in hypoperfusion of cells. This results in cellular hypoxia, generating anaerobic metabolism and increased oxygen demand. A disturbance in acid-base balance stimulated the respiratory centre in the medulla oblongata resulting in increased respirations to meet increased oxygen demand – TACHYPNOEA (Respiration Rate of over 20 breaths per minute)
(Steen 2009)
The hypothalumus is stimulated by the widespread blood-borne infection and microorganism invasion . An increase in temperature is the patients own body defence in fighting infection. Resulting in PYREXIA (core body temperature of over 38degrees Celsius) (Creed & Spiers 2010)
The patient will appear flushed, warm to touch and sweating. The flushed, warm peripheries , redness is a result of the widespread vasodilation and reduced osmotic pressure. This causes the oedema in the interstitual spaces (Creed & Spiers 2010)
Widespread vasodilation causes a disturbance of blood flow within the cardiovascular system. Vasodilation is caused by nitrous oxide production stimulated by cytokines which are released in the inflammatory response. As the lumen of the vessels dilate it is difficult to maintain adequate blood pressure causing reduced systemic vascular resistance (SVR). The heart tries to compensate by increasing its cardiac output and a tachycardia may be detected (Heart Rate of over 90 beats per minute) (Steen 2009)
The pulse may feel bounding and full and the patient can be described as being in th e hyperdynamic phase (Creed & Spiers 2010).
Stage 3 – Hypodynamic Stage
If the pressure of blood perfusing the kidneys drops, they respond by releasing renin which activates the angiotensin mechanism. Angiotensin has a powerful constricting effect on the vessels, resulting in increased blood pressure. It also promotes the conservation of water and salt by the kidneys, both of which preserve or increase plasma volume. Falling blood pressure also causes the release of the anti diuretic hormone. This conserves water in the plasma resulting in REDUCED URINARY OUTPUT (Moore & Woodrow 2009)
Interruption of renal homoeostasis can lead to chemical disturbances and the body can no longer excrete waste products such as urea. Uraemia adversely affects the Central Nervous System (CNS) resulting in REDUCED LEVELS OF CONCIOUSNESS
This also is a result of inadequate cerebral perfusion.
As sepsis develops into the hypodynamic stage this means that the hyperdynamic stage can no longer be maintained.
The patient physiological reserve becomes exhausted the blood pressure becomes decompensated and falls to inadequate levels. The patient will be hypotensive with a systolic blood pressure of
The cardiovascular system is compromised as the myocardium becomes hypoperfused, there is myocardial depression with reduced cardiac output.
Peripheral vasoconstriction will reduce the volumes of blood perfusing the peripheries, reducing blood flow to the hands and lower parts of the legs.
The patient will give rise to PALLOR with COLD & CLAMMY SKIN. The skin may also appear mottled.
A drop in blood pressure causes the patient to by clammy. This is caused by a cold sweat occurring in the absence of an increased body temperature.
Stage 4 – Late hypodynamic stage progressing to organ dysfunction and severe sepsis
In the later stages of sepsis, developing into severe sepsis, the myocardium becomes more and more depressed and it may be almost impossible to feel a peripheral pulse (Creed & Spiers 2010).
Inadequate renal perfusion resulting in depressed Glomerulus Filtrate Rate (GFR) there may be oliguria, which is production of abnormally low urine volumes and in some cases anuria which is the total absence of urine.
As the kidneys are not producing urine this will give rise to pulmonary oedema – the patient may appear dyspnoeic with basal crackling breathe sounds during respiration. There may also be raised jugular pressure.
There will be severe neurological dysfunction due to production of waste products from renal failure, hypoperfusion – hypoxia and the production of lactic acid in anaerobic metabolism and fluid overload (cerebral oedema). Resulting in reduced levels of conciousness and raised intracranial pressure.
907 words
References
Bacidore, V. et al (2009) A Collaborative Framework for Managing Pregnancy Loss in wwwEmergency Department. Journal of Obstetric, Gynaecologic, & Neonatal Nursing. 38 (6) p.730-738
Creed, F. & Spiers, C. (eds) (2010). Care of the acutely ill adult: an essential guide for nurses. Oxford: Oxford University Press.
Crouch, R. (ed) (2009). Oxford handbook of emergency nursing. Oxford: Oxford University Press
Fischerova, D. (2009). Urgent care in gynaecology: Resuscitation and management of sepsis and acute blood loss. Best Practice & Research Clinical Obstetrics and Gynaecology. 23 (5) p.679-690
Garretson, S. & Malberti, S. (2007). Understanding hypovolaemic, cardiogenic and septic shock. Nursing Standard. 50.(21) p.46-55
Higginson, R. & Jones, B. (2009). Respiratory assessment in critically ill patients: airway and breathing. British Journal of Nursing 18.(8) p.456- 461
Jones, B., Higginson, R. & Santos, A. (2010). Critical Care: assessing blood pressure circulation and intravascular volume. British Journal of Nursing 19.(3) p.153-158
Jevon, P. (2010) ABCDE: The Assessment of the critically ill patient. British Journal of Cardiac Nursing. 5 (8) p. 268-272
Kisiel, M. & Perkins, C. (2006). Nursing Observations: knowledge to prevent critical illness. British Journal of Nursing. 15 (19) p. 1052-1056
McLeod, A. (2004). Intra- and extracranial causes of alteration in level of consciousness. British Journal of Nursing. 13.(7) p.354-361
Moore, T. & Woodrow, P. (2009) High dependency nursing care: observation, intervention and support for level 2 patients. 2nd Ed. Abinsdon: Routedge.
NHS Evidence (2009) Emergency and Urgent Care: Defining sepsis, severe sepsis and septic shock. [Online]. October 2009. Available from: http://www.library.nhs.uk/emergency/viewresource.aspx?resid=269236. Accessed 25th November 2010.
Oldham, J Sinclair, L Hendry, C (2009) Right patient, right blood, right care: safe transfusion practice. British Journal of Nursing. 18 (5) p. 312-320
Resuscitation Council (UK). (2010) Resuscitation Guidelines. October 2010. [Online]. Available from: http://www.resus.org.uk/pages/GL2010.pdf. [Accessed: 9th December 2010]
Santy, J (2008) Recognising wound infections. Nursing Standard. 23 (7) p.53-60
Scottish Intercollegiate Guidelines Network. (2004). Postoperative Management in Adults: A practical guide to postoperative care for clinical staff. No. 77. [Online]. August 2004. Available from: http://www.sign.ac.uk/guidelines/fulltext/77/index.htm. [Accessed: 10 November 2010]
Steen, C (2009) Developments in the management of patients with sepsis. Nursing Standard. 23 (48) p. 48-56
Vuolo J C (2006) Assessment and management of surgical wounds in clinical practice. Nursing Standard. 20 (52) p. 46-56
World Health Organisation (2009) WHO Guidelines for Safe Surgery 2009: Safe Surgery Saves Lifes. September 2009. [Online]. Available from: http://whqlibdoc.who.int/publications/2009/9789241598552_eng.pdf. Accessed: 30th November 2010.
Part B – Question 2a
Mr Henderson has arrived in hospital after a history of falls at home and has just commenced a new medication regime.
It is very possible that he may be anxious, worried, frightened as a result of falling at home which also may result in loss of confidence. He may also be apprehensive about his new medication regime. Having been diagnosed with Parkinson’s for 5 years, he may already know the importance of getting his medications on time, in reducing the symptoms allowing him to maximise his independence. However, it is not for the nurse to presume this and she/he must sit down, talk to him, allowing him time to talk and express his worried and anxieties. This was help to establish a relationship and Mr Henderson will understand that you are there to support him throughout his journal of care (Walsh & Crumbie 2007). The nurse should also make sure that all members of the multidisciplinary team are aware of Mr Henderson’s condition and if they are not aware of the importance of getting medication on time out (Sadler 2007) with ‘normal’ drug rounds then they should be informed of its importance and understand the significant consequences resulting from not getting the drugs on time such as reduced independence and prolonged hospital stay. As medications are a large part in maximising independence and mobility and it may be suggested that Mr Henderson receives his medications before getting out of bed in the morning. This will allow time for the drugs to work and therefore enabling him to get out of bed more easily.
‘Freezing’, a symptom of Parkinson’s’ disease can be distressing for patients. It affects gait initiation, turning and moving through small spaces, such a doors and busy areas (Axer 2010).. Anxiety can exacerbate freezing and it is vital that the nurse can firstly recognise anxiety, this may be achieve through effective communication and listening skills and secondly developing strategies to reduce anxiety levels such as allowing him time to talk, listening and taking on board his expressions allowing for a trusting relationship to be developed, helping him to build in confidence and preparing him psychologically for going home. Various strategies have been suggested to assist with ‘freezing’. Alexander, Fawcett & Runicnan (2006) suggest cognitive techniques in breaking down movement. They suggest breaking down the task of getting out of bed in the morning and describe that patients should bend their knees so that feet are flat on the mattress and they the patient should swing knees in the direction that he wants to turn. The next stage can involve clasping both his hands and lifting them straight up, straightening the elbows, then turning the head and swinging the arms in the same direction as the legs. Finally the patient can grip the edge of the mattress and adjust his position until comfortable. When Mr Henderson is mobilising then it is important that he does not have any distractions and the nurse or other members of staff should not disturb or interrupt if at all possible as this could lead to ‘freezing’. The Parkinson’s Disease Society (2007) describe cueing strategies as external meaning visual, auditory or preprioceptive or internal meaning cognitive.
Visual cues could be stepping over a cue in the floor, for example tape can be placed on the floor in strips to help initiate in conf
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "pneumothorax"
Patients can develop a pneumothorax from various means and either (primary or secondary) can occur spontaneously. A primary pneumothorax is reserved for those without any underlying lung pathology, while the term “secondary” pneumothorax is used clinically to indicate patients that carry an established diagnosis of lung disease.
Related Articles