The aim of this essay is to reflect on how I have become competent in a particular clinical skill. The clinical skill I have selected is administering intramuscular (IM) injections. I will provide a rationale for choosing this skill and use appropriate literature to demonstrate my knowledge underpinning this skill. Although there are five sites for administration of IM injections, for the purpose of this essay I will discuss only two of the sites. Firstly, the dorsogluteal (DG) site as this is the site I used when giving IM injections in line with the local trust policies and procedures. Secondly I will discuss the ventrogluteal (VG) site, as recent literature has shown this site to be the safest to use when administering IM injections. I will then reflect on my learning and how I have become competent in this area.
There is a need for nurses to be skilled in the administration of intramuscular injections in the learning disability field. The National Institute for Health and Clinical Excellence (NICE) (2006) suggests that when de-escalation and intensive nursing techniques have failed to calm the patient and they are at risk of harming themselves or others, then rapid tranquillisation should be used as a last resort. Although oral tranquilisation will be offered first, due to the high state of aggression, agitation or excitement the patient may be unable to give their consent. Therefore the 1983 Mental Health Act and the guidance on Consent to Treatment (DH 2002) must be followed. Consequently, rapid tranquilisation will be achieved by the administration of medication through IM injection to control severe mental and behavioural episodes and to calm the patient quickly.
Greenway (2006) suggests that IM injections are generally likely to happen in association with the administering of antipsychotic medication in the form of depot injections and/or rapid tranquilisation, for managing mental illness and/or challenging behaviour for people with a learning disability. Greenway also implies that there will only be a small number of learning disability nurses that will actually use the skill of administering IM injections after they have qualified, due to a decline in depot administration. However, the Nursing and Midwifery Council (NMC) (2004) identifies that the role of the learning disability nurse is forever changing and the administration of injections will depend on the client group and the practice areas in which they work. They recognise that it is a key challenge for learning disability nurses to update their knowledge and maintain competence in a skill that they may use infrequently. Irrespective of this, the clinical procedure should be developed and maintained in line with evidence based practice, regardless of how often it is used.
The administration of IM injections is a vital component of medication management and is a common nursing intervention in clinical areas. Less pain to the patient and unnecessary complications can be avoided by the nurse being skilled in the injection technique used (Hunter 2008). The National Patient Safety Agency (NPSA) (2007) notes that the injecting of medication is complicated and patients can be put at risk. Incompetency, lack of training and varying knowledge levels of nurses were factors highlighted in errors made around injecting medicines.
Adhering to the aseptic technique during preparation and administration of the injection, and inspecting the injection site for any signs of skin deterioration are vitally important to prevent infection and complications (Dougherty 2008).
Alexander et al (2009) describe the correct way to give an intramuscular injection in the DG site using the Z tracking technique.
Using the thumb or the side of the non-dominant hand stretch the skin taught over the site of injection maintaining the tautness during the procedure.
With a darting motion, insert the needle at 90 degrees to the skin, 2-3mm of the needle should be exposed at the surface and the graduation marks on the syringe barrel must be visible throughout.
Use the remaining fingers of the non-dominant hand to steady the syringe barrel, whilst using the dominant hand to pull back on the plunger to aspirate. If blood appears all equipment should be discarded and the procedure should be started again. It is safe to carry on if no blood appears.
The plunger should be depressed at a rate of 1ml per 10 seconds to give the muscle fibres time to expand and accommodate the drug.
After a further 10 seconds remove the needle and then release the traction on the skin.
The injection site may be wiped with dry gauze if need be.
A plaster can be applied if the patient requires and if they have no known allergy to latex, iodine or elastoplasts.
Controversy lies around the site area chosen for administering the IM injection. Although the DG site is the traditional choice by nurses for the administration of IM injection there are risks associated with this site of injection. The DG site is situated in the upper outer quadrant of the buttock and is often landmarked by visually quartering the buttock horizontally and vertically, then repeating this action in the top right hand square. Evidence shows that the use of this site for IM injection can run the risk of injury to the sciatic nerve and the superior gluteal artery (Small 2004). Additionally it can cause skin and tissue trauma, muscle fibrosis and contracture, nerve palsy and paralysis as well as infection (Zimmerman 2010).
The belief by nurses that the VG site is hard to landmark suggests reluctance on their part to change a practice they are competent in. Although once nurses have become familiar with location of the VG site and the surrounding anatomy, they will become confident in using this site (Greenway 2006). Hunter (2008) suggests to locate the VG site the nurse should place the palm of her right hand on the patients left hip (the greater trochanter), then make a ‘v’ by extending the index finger to the anterior iliac spine. The injection is given in the middle of the ‘v’ in the gluteus medius muscle. Administering IM injections using anatomical features leads to a more specific and correct way of carrying out the procedure.
In contrast to the DG site, the VG site has no major complications associated with the administration of IM injections. Zimmerman (2010) also strongly advocates the use of the VG site. Although there appears to be a lack of current evidence for choosing the VG site rather than the DG site for rapid tranquilisation during restraint of a patient. Because of the nature of the situation during this procedure, safety for all involved has to be considered. Local policies should be utilised for specific guidance on positioning the patient safely and for use of specific holds needed to allow the VG site to be landmarked and the injection administered. The VG site can be used if the patient is prone, semi-prone or supine (Greenway 2006).However, following a literature review of damage to the sciatic nerve from IM injections, Small (2004) recommends that the VG site should be chosen over the DG site for IM injection. Zimmerman (2010) concurs with this, strongly advocating the use of the VG site for IM injections of more than 1ml in patients over the age of seven months.
More evidence for choosing the VG site is a study carried out by Nisbet (2006) showing that the subcutaneous fat level of the DG site is significantly higher than that of the VG site. It also showed that penetration of the target muscle at the DG site was only 57 percent meaning the remainder of the injection would deposit into the subcutaneous fat leading to a deficit in the uptake of the drug. Emerson (2005) reports an increased risk of obesity in people with a learning disability. In one study 90 percent of adult females and 44 percent of adult males had fat deposits in the DG site area that were one inch deeper than the shorter IM needles would reach (Zaybak et al, 2007). The VG site has a shorter distance to the targeted muscle and is a safe alternative choice for the administration of an IM injection, Greenway (2006), Small (2004) and Zimmerman (2010) suggest it is time for professionals to rethink the site of IM injections in people with a learning disability.
I will now discuss how I have become competent in carrying out this clinical skill and to do this I will use a reflective model. Reflection is a way in which nurses can bridge the theory-practice gap. The process of reflective practice allows the nurse to explore, through experience, reflection and action, areas for developing their practice and skills. It is an important part of gaining knowledge and understanding. The use of a recognised framework allows for a more structured approach when reflecting upon practice (Johns, 1995).
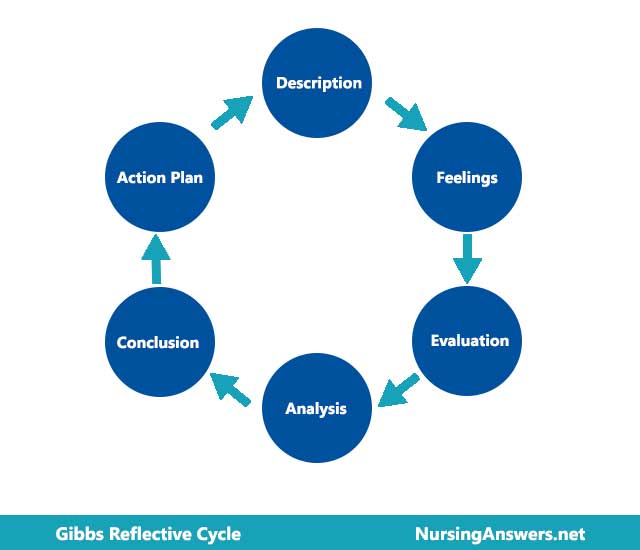
I have decided to use Gibbs (1998) Reflective Cycle, as it provides a straight forward and structural framework and encourages a clear description of the situation, analysis of feelings, evaluation of the experience, analysis to make sense of the experience, conclusion where other options are considered and reflection upon experience to examine what the nurse would do should the situation arise again.
In describing what happened in learning this skill the theory of experiential learning can also be used as a framework. The theory of experiential learning was developed by Steinaker and Bell (1979). The Experiential Taxonomy highlights 4 levels of learning that the nurse will go through in learning a new skill i.e. exposure and participation, identification, internalisation and dissemination.
During exposure there is a consciousness of the event and the nurse will have observed a competent practitioner carry out the task. In this case I had an awareness of needing to be able to administer IM injections competently due to the client group involved. In my first week of placement I observed a qualified nurse administering PRN and depot IM injections several times while the nurse talked me through the procedure step by step. As she was demonstrating the procedure and talking me through it my thoughts and feeling at the time were that I would not be able to remember all the steps needed to administer the IM injection safely and I was also feeling anxious about potentially causing pain and/or injury to the patient. Participation involves the nurse becoming part of the experience. After observing the practice I participated in the drawing up of the injection and then administering it.
Identification involves the nurse becoming competent in the skill. On reflection as soon as I started on placement I realised that I would have to gain as much experience as I could administering IM injections, not just the actual procedure of giving the injection but also the knowledge to underpin this skill.
Internalisation occurs when the new skill becomes part of everyday routine. Several weeks into my placement I felt that I had eventually become competent in administering IM injections, my anxieties began to lessen and I started to feel more confident that I was becoming proficient in carrying out the procedure. I found that the more times I carried out the procedure the better I felt about it.
Dissemination involves the nurse being able to influence others and showing others how to carry out the skill. Although this was only my second placement I feel totally competent in carrying out the task. I also feel that I have a good understanding of the underpinning knowledge involved. Therefore I feel I would be able to teach others how to do this.
On reflection I do not think I would have learned this skill any other way, I have realised that initial anxieties about carrying out a new task are usual. But I will have to remember this will pass as I practice more and become more experienced.
I have also realised through reflection the importance of having underpinning knowledge in relation to clinical skills and understanding why we do things rather than just simply learning how to do them.
In conclusion, this assignment has explored one clinical skill in which I have gained competence. A rationale was provided in that IM injections are an important part of everyday life for the client group involved. IM injections are considered to be a routine procedure, it is a valuable and necessary skill for nurses. To provide safe practice and ensure accurate and therapeutic drug administration, the nurse should use clinical judgement when choosing the injection site, understand the relevant anatomy and physiology, as well as the principles for administering an IM injection. By using a reflective model and theory in relation to experiential learning I have discussed my own personal and professional development in terms’ of my knowledge and skill acquisition in this area of clinical practice.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gibbs reflective cycle"
Gibbs' Reflective Cycle was developed by Graham Gibbs in 1988 to give structure to learning from experiences. It offers a framework for examining experiences, and given its cyclic nature lends itself particularly well to repeated experiences, allowing you to learn and plan from things that either went well or didn’t go well. It covers 6 stages.
Related Articles