Provide an in-depth reflective account that demonstrates how learning, during the three years of the child nursing course, has been achieved in relation to two areas of your practice which has informed and enhanced your development towards qualification as a Children’s Nurse.
Introduction
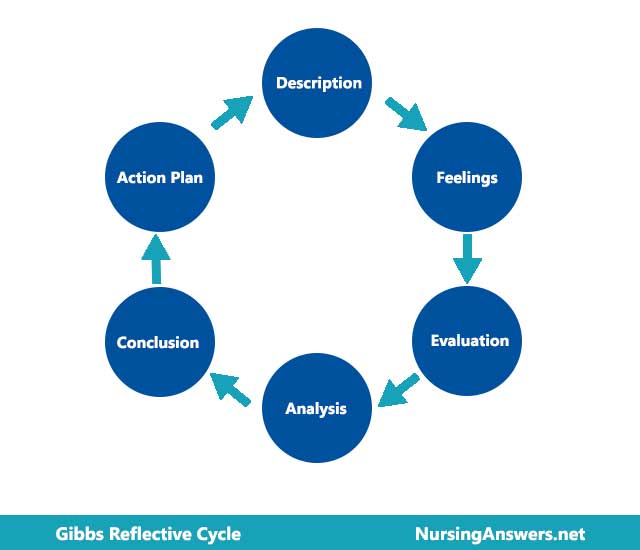
Reflection is a vital component of the development of nursing competence and reflexive nursing practice. Although reflection functions on many levels, including the personal level, in allowing student nurses to review experiences and incorporate them into their internal schema, one of the most important levels of reflection is the process of asking questions about practice, and through asking those questions learning about the self in practice, and the role of the nurse (Bowden, 2003). Reflection is an important aspect of developing competence in practice, as well as developing practice itself (Durgahee, 1998; Gustafsson and Fagerberg, 2004). Some authors view the ability of the nurse to reflect on practice and in practice as a fundamental component of providing truly holistic and client centred care (Gustafsson and Fagerberg, 2004), while others view reflection as a self-limited, flawed and biased practice which is of little or no use to developing nursing professionalism (Jones, 1995). I believe that reflection, if properly used and structured, provides powerful insight into the self, into practice, and into the ways in which competence and practice develop over time and through experiential learning. Therefore, I have concluded that to make reflection effective and useful, it is important to use a reflective model, such as that of Gibbs (1988), which I have chosen for this essay. Although there are limitations to Gibbs’ (1988) model, particularly in applying it to the requirements of this essay, it provides clear guidance and useful questions to ask about the experiences that contribute to the reflective process. I have adapted this cycle to suit the processes and analyses of this essay, and so, while two cycles of reflection are outlined below, the conclusions are developed collectively. For the purposes of this essay, the final stage of the cycle is to be found within the Appendix (see Appendix 1), and thus the Action Plan is adapted to become the Personal Development Plan.
The purpose of this essay is to engage in an in-depth, detailed process of reflection on two areas of practice and learning that have been important to me through my studies in the three year child nursing course. Using a reflective cycle to guide and direct the reflective process, I will explore the process of professional development, towards competence and expertise, in relation to Benner’s (1984) stages of development, examining the nature of competence in each designated area of practice.
The first chosen area of practice is the skill of managing an intravenous infusion, because the use of intravenous infusions and the provision of intravenous medications is an important component of many clinical paediatric nursing scenarios, and the management of intravenous access and infusions is particularly problematic when nursing children. The other area of practice and nursing professionalism chosen is communication, with a particular focus on the development of communication skills with staff, in relation to the nursing handover within the acute hospital environment, and the development of communication skills with patients, using the example of providing health education and promotion for a patient with Type 1 diabetes. I have chosen to focus on specific examples of communication skills in practice because these relate strongly to my own experiences, and also allow for a deeper and more critical analysis of practice and my own development. This will also allow for a more concrete development of a personal development plan to encompass identified development needs and actions to achieve these during the first six months of practice as a Registered Children’s Nurse.
The focus on critical analysis allows for the development of a skill of great value for my professional practice, deconstructing practice and reviewing it in the the light of other knowledge (Burns and Bulman, 2000). However, because of the complex nature of practice, and the reflective processes which question feelings and thoughts as well as actions, the reflective process is complex (Wilkinson, 1999). Thus, although there are two issues being reflected upon, they are drawn together in one discursive thread which signposts the learning and development, the acquisition of professional understanding, which signifies the transition from novice to competent practitioner.
Discussion
1. Clinical Skill Development: Intravenous Infusion and Medication Management in Children’s Nursing Practice.
Description: What Happened.
During the three years of nurse training, the development of the skill of managing intravenous infusions, either of hydration solutions or of medications, was one which I developed almost from the beginning, when it was taught as a clinical skill in the university setting. The typical approach to teaching clinical skills was to provide the students with a lecture on the relevant theory, complemented by a practical skills session to apply the knowledge in a simulated environment, utilising mannequins. Every acute ward area of my clinical practice involved the care of patients with intravenous infusions, which included caring for children while the intravenous cannula was inserted, and then monitoring and care of the intravenous cannula site, and of the infusion itself. This skill was therefore not only a basic skill for nursing competence throughout my training, but also an important opportunity to promote health, prevent infection, and was fundamental to other aspects of care and treatment.
Over the three years, I first learned how to set up an intravenous infusion, safely and in a sterile manner, how to check the infusion, and how to check the infusion rate manually (ie, without the use of an infusion pump, although infusion pumps are standard best practice in children’s nursing). During clinical practice, I learned how to support a child during the cannula insertion, monitor the site, check the infusion and infusion rate, set up and check different types of infusion pumps, and how to change the IV line (which must be changed regularly). I also learned complementary skills such as drug and dosage calculations for infusions, and fluid balance calculations, both of which required numeracy skills
Feelings: what were you thinking and feeling?
Throughout my training, management of intravenous infusions was stressful, but in particular, the associated aspects of care were challenging. Supporting children who have intravenous infusions is problematic, particularly as the experience is often painful and distressing for them. Carrying out drug calculations was terrifying at the beginning of my training, and even by the end, despite increased competence and confidence, I would still have more than one colleague check calculations and dosage rates, and check infusion rates on pumps, to ensure I had made the correct calculations. I felt very lacking in confidence in this area. I also felt that while I focused on safety aspects of IVI use, including risk management and prevention of infection via the IV site, other colleagues did not seem to pay so much attention to this aspect of care.
Evaluation: What was good and bad about the experience?
It was good that I identified important aspects of this clinical skill, and the complexities of practice surrounding it. What was not so good was the lack of transparency in colleague’s practice, particularly in my earlier clinical placements.
Analysis: What sense can you make of the situation?
I became aware during my reflection on this element of my learning that it was very much something which became assimilated into the almost intuitive elements of nursing competence (Benner, 1984). This was because apart from the elements of the process which had been identified as distressing for the child, such as cannula insertion and removal, managing the IVI had become ‘second nature’, and checking the line, site and rate of the pump were activities that the qualified nurse carried out without any overt signifying of the action, as part of her interactions around the patient/bedside. Thus, making this overt was almost counter-intuitive. Certainly, it appeared to me that many staff did not record these observations every time they were made, and that they did not always communicate these observations to others, including me, as a student. As a student, a learner, I was required to take more time over such observations, to note their significance, and to evaluate their place within my nursing work. I was required to develop specific skills around the use of IV infusions and the management of whatever medication or fluid was being infused. This was a protracted learning process, which developed throughout the three years. I learned the importance of this for my practice. “Possible complications associated with short peripheral
venous access include infiltration of infused fluids (nonvesicants) into the surrounding tissue, extravasation of vesicant medications or blood into the surrounding tissue, and phlebitis” (Hinkle and Hadaway, 2006 p 122). The clinical skill here also, therefore, included the component of determining when such complications had occurred. I also had to learn to observe for infusion reactions, which could range from mild to severe (Hinkle and Hadaway, 2006).
Competency can be viewed as behaviours which are achieved or approved of in relation to the completion of a task, and competency is described in relation to that task (Gonczi, 1993). However, developing competence in IVI management is much more than simple task proficiency, and this may be true of much of professional competence in nursing (Preston and Walker, 1993). Not only does it appear that no single clinical requirement can be reduced to single task, but also, competence in that task may be affected by other contextual factors, including the presence of others, and how their contribution or lack of it can affect performance of clinical actions (Ashworth and Saxton, 1990). If we view competence as the ability to manage any situation holistically, making use of collaboration with colleagues (Meretoja et al, 2002), then even this process of reflecting on a clinical skill is very limiting, because the skill alone does not signify the whole of the learning process associated with that area of practice throughout my training. One of the important elements of learning around this particular skill, however, was the gradual recognition of my own competence, which was signified most clearly when I no longer become ‘overt’ about assessing the IVI and monitoring it, but carried out this activity as part of my practice, almost automatically. Here, the skill had many facets, but this kind of ease was never achieved with the drug/dosage/infusion rate calculations.
Numeracy competence is important for nurses, and nurses are required to demonstrate acceptable levels of numeracy in order to qualify (Bath et al, 1993). However, this was an area I struggled with, not because I had ever considered I had difficulties with numeracy, but because applying numeracy to clinical situations seemed to make drug calculations much harder. Over time, I found that if I visualised the calculations myself first, and wrote them out longhand, then checked them with a calculator, I usually reached the right conclusion, which showed that my own learning style influenced my ability to come to the right answer(Bath et al, 1993; Galligan, 2001).
Hinchliff (2004) descrives Bloom’s (1972) learning domains, and this learning experience, throughout the three years, involved all three areas: cognitive, psychomotor, and affective. In relation to the cognitive domain, I learned knowledge to underpin practice, consolidated this knowledge over time. In relation to psychomotor skills, these were about the practical ability to carry out necessary procedures and actions, including running fluids through an IV line, identifying, choosing, priming and setting up the correct line for the correct infusion pump, and the skills around removal of the cannula and dressing of the cannula after insertion, along with changing an IV bag. The affective domain refers to the attitude formation, which can be seen above to be about a positive attitude but an internalisation of much of the knowledge and practice to the point that aspects of these procedures became almost innate.
It became apparent that this clinical skill could not be viewed in isolation, and also incorporated a great deal of discussion with the family and the patient, and in the case of most children, informing them of the need to take care of the IV line, and educating them about infection control, thus engaging them in their own care and in their own health promotion (Long et al, 2008). Prevention of trauma to the IV cannula or site, and ensuring maintenance of patency of the cannula and line, are important in minimising the amount of times the cannula needs to be resited, which is desirable because of how distressing this procedure is for most babies and children (Thomas, 2007). I became aware of this after viewing resiting of cannulae in a number of patients, most often due to either traumatic accidental removal.
2. Professional Skill Development: Communication in Practice: The Nursing Handover.
What Happened
During the three years of training, communication was identified as a professional skill, and it soon became apparent that this skill formed the basis of the majority of nursing actions and roles. Because of the complexity of communication in nursing practice, during this reflection I chose to focus on one aspect, that of providing handover for a designated patient, or group of patients, under my care, to the nurse taking over care. Engaging in this activity was a significant aspect of my development. Initially, in the first clinical placements, I observed this taking place, but did not really understand all the components of the process. Over time, I was encouraged by mentors to provide the handover report myself, and I found this demanded communication and information processing skills perhaps unique to the process and to the situation. I discovered that I needed to know the terminology and abbreviations used, the format of the report, and to remember the patient information and provide a comprehensive report that did not omit important elements of care. During the initial experiences of this, I did miss out elements of care, but was always supported by a mentor who could augment my limited report and ensure patient needs were communicated. However, by the end of my clinical experiences I was expected to provide reports myself, and I did so, but became increasingly aware of the limitations of this form of communication, and of how it had become ritualised in practice (Strange, 1996). Understanding the nature of this element of communication became an important element of my learning, perhaps because I had found it so difficulty initially
Feelings: what were you thinking and feeling?
During successive experiences of handover, I came to a growing realisation that the format and nature of the handover report was not only extremely ritualised (Strange, 1996), but also constituted a unique form of communication, with certain expected behaviours and standardised formats. However, I started to feel, quite early on, that information was not necessarily being fully communicated, and I found myself increasingly frustrated with the process, because instead of providing a comprehensive report, it was more a kind of focused tick list of tasks, which did not really relate to my concept of holistic approaches to nursing care. I found myself learning how to give a ‘proper’ handover but wishing I could give a ‘good’ handover.
Evaluation: What was good and bad about the experience?
The good aspects of this experience were the fact that I was able to identify what was happening, and able to realise that I was frustrated with the process of handover, and the way it had become habitual. This prompted me to explore the evidence base surrounding this important aspect of nursing communication, which then enhanced my understanding. However, to cite what was bad about the experience, I must focus on the limitations of the process, because it made me feel that the handovers were, quite often, inadequate, and very limited, reducing patients to a list of problems and actions. Having said this, it also became apparent that handovers conducted at the patient’s bedside were an entirely different entity, and that communicating at the bedside included the patient and their family in the handover, and made them much more holistic and comprehensive. But it may not be appropriate to do this in all situations.
Analysis: What sense can you make of the situation?
Developing professional skills is part of the complex acquisition of nursing competence, and this process can be viewed as an apprenticeship of sorts (Benner, 1984). Much of the professional competence that is assessed during nurse training is related to the standards set out by the Nursing and Midwifery Council (NMC, 2004), and are realised through a process of learning, negotiation and assessment which predominantly occurs through clinical practice. While a lot of this learning is directed and planned, development is through experiential processes, as in this case, in the development of the required verbal communication skills for providing ‘handover’ report. This emerged as a significant area of practice for me, particularly in relation to responsibility and autonomy after the transition from student nurse to staff nurse, because of the different expectations of the latter role. While in relation to performance, clinical skill and professional skill, the senior student nurse and the newly qualified staff nurse are similar, in relation to role and responsibility, and expectation, there is a sudden shift and competence takes on new meaning for the newly qualified nurse (Wade, 1999). Thus, I can see that my concerns about the nursing handover, and my ability to provide an appropriate, comprehensive report, were very clearly linked to this notion of responsibility, because a poor handover could impact on patient care (Sexton et al, 2004).
The nursing handover report is a process which involved the communication of key information about patients on the ward, care plans, actions and imminent needs, and about the stage of their care journey (McKenna, 1997). It usually occurs as a communication between nurses at the point of shift change (McKenna, 1997), but it can also take place when a patient is transferred from one clinical area to another. According to Hopkinson (2003) the nursing handover is an important and significant activity in the hospital setting, relating to the proper management of care and the provision of continuity of care (Kerr, 2002).
Although handovers have the same basic function, I have observed that they can vary from ward to ward, but that within each location, they seem to have a certain format or shape. While in some areas tape recorded handovers are used, in others, the staff provide a handover at each bedside. More commonly, handover occurs in a designated room (to ensure confidentiality), and may then in some circumstances be followed by a ward round to introduce the next shift to the patients and their family. It is important to include the family in this communication, because most sick children are accompanied by a parent or carer during their stay in hospital, for a large proportion of the time. The nurse may either hand over the care of one patient, a group of patients, or the entire ward, if they have been the nurse in charge of the ward for that shift. This requires that the nurse providing the report must have a thorough and comprehensive knowledge of the patients, their needs and diagnoses, treatments, and any pending results or procedures. Not only is it a process of communicating this information, it is also the time when colleagues might ask questions about care, and therefore also serves to demonstrate what the nurse has achieved, or not achieved, during the preceding time period, and tests the nurse’s knowledge of the patients. Yet some evidence suggests that handovers are limited and undermined by forumulaic approaches to providing the information, by incomplete communication, use of cryptic terminology, jargon and abbreviation, and can require that nurses have ‘socialized knowledge’ in order to understand them (Payne et al, 2000). Thus, it can be difficult for the student, or even the newly qualified staff nurse, to fully understand this communication because they perhaps are not fully socialised into the clinical area. Terminology and units of language may acquire different significance in specific areas of practice (Payne et al, 2000). Another identified limitation is the tendency to prioritise biomedical and physical aspects of care, reducing the patient to their disease and its treatment (Payne et al, 2000).
The handover forms the initial part of the process of care planning for the nursing staff taking over care, although this is supplemented by a thorough examination of the patient records, and discussion with the patient and family. Having observed and participated in such processes, it is understandable that this communicative act developed some significance for me in relation to professional development, particularly in relation to future practice as a qualified staff nurse. Competence takes on new meaning at this transition (Amos, 2001; Ashworth and Saxton, 1990), because it signifies the point when I have to become responsible and accountable for my own actions, with no one else to cover any inadequacies or mistakes (Gerrish, 2000). Because it is viewed as a fundamental component of good quality nursing care (Pothier et al, 2005), ‘getting it right’ is understandably important.
Handover can be viewed as a communicative act from a number of perspectives. It provides a forum for discussion, debate and questioning, as well as expressing one’s views and feelings about a particular case or cases (Hopkinson, 2002), which to me suggests that it is more than simply the presenting of information, but is also a form of self-expression for the nurse. However, it’s main purpose is to provide the information that nurses will then use to formulate their plans for care and their prioritisation of their workload for that shift (Hopkinson, 2002). For example, in one handover a colleague did not inform staff that a chest X-ray had been carried out, which meant that the next shift ordered another chest-X ray with resultant delays and confusion.
Providing a good quality handover may be more significant than ever in the current clinical paediatric nursing environment, where every aspect of healthcare appears to have become more complex, requiring more multiprofessional input and collaboration, and in which patients are subject to complex and multifactorial assessments (Pothier et al, 2005). There is some evidence to suggest, however, that important patient information can be lost during the shift handover (Pothier et al, 2005), which reinforces my own conclusions about this communication. This may not, however, be due to simple acts of omission, but also due to the culture of ward areas and the ways in which nurses behave and exercise power, albeit a small degree of power, over the information they possess (Hardey et al, 2000). Some research suggests that the handover process is where tensions an institutionally-derived conflicts and drivers for nurses can become evident (Parker et al, 1992). It would seem that it is more than a simple process of dialogic communication (Kerr, 2002), but also serves a range of other functions, including social and protective functions (Strange, 1996). To me, this knowledge and understanding of the deeper and wider aspects of communication, of what is being communicated, how and why, during this process, signifies the journey of learning and development as a student nurse. Initially, I was the novice, viewing this process as a mere interchange of key information. Gradually, however, I developed an intuitive knowledge of the handover and its communicative role, intuition based on experience and on the processing of a range of cues and sources of information (Benner, 1984), leading to a degree of awareness that the handover signified more than simply an exchange of facts. It demonstrates competence in communication, but in adherence to cultural roles and expectations, and the ability to mange the competing demands and tensions of the nursing role (Kerr, 2002). Thus it emphasises a shared valued system amongst the nurses within the given context (Lally, 1999), which in some ways can demonstrate competence and acceptance, of me by qualified colleagues, signifying I have achieved nurse status, but also which can mean an enforced compliance with local behaviours and expectations which may be at odds with my own philosophy and principles of professionalism. Therefore, I realised that the communication skills of the nursing handover are both verbal and personal, involving managing myself, managing information, and managing the work environment and my colleagues (Lathlean and Corner, 1991).
Achieving competence in the effective verbal communication skills associated with the handover is problematic, because from all that I have learned through my education, and my exposure to the ideals of professional nursing, the handover should be a detailed, comprehensive communication delivered without jargon or abbreviations, and which is inclusive of the patient and their carers. However, the conventions of the handover in different areas may oppose this. This is an area of development identified as important for my personal development plan.
Conclusions
The first conclusion I draw from this reflection is that it is impossible to see any area of nursing competence, or any clinical skill, as a discrete entity or area of practice. Every skill and professional role is inextricably linked with others, with aspects of practice, with other skills, demonstrating the complexity of practice and of the learning and development processes which lead me towards expertise and confidence, as well as basic competence. As I have demonstrated above, managing an intravenous infusion involved a range of skills and actions, including numeracy calculations, risk management and prevention, health promotion, patient support and education, care planning, and communication. Thus, it becomes evident that what may be identified as a discrete clinical skill intersects with multiple areas of practice and competence. This perhaps reflects holistic models of nursing, because it demonstrates that the nurse cannot deconstruct practice to such an extent as to make it fully task oriented, due to these intersections and the interconnectivity of different tasks. It would appear, from my reflections, that the ideals of ‘holism’ which are expounded in relation to nursing ideologies and philosophies can be viewed on the ‘micro’ level in practice, as well as the ‘macro’ level of the nursing philosophy. Every part of clinical practice is an element of a complex, yet connected, ’whole’, and therefore, competence in every part of practice is important in order to provide optimal standards of care in every respect. This is an important realisation for me, and one which I believe to be appropriate for this stage of my development. It might be that coming to this realisation earlier on in my professional development journey would have been too overwhelming. Coming to this realisation now, when I can signpost my own learning, development and competence, is more motivating than challenging, because it underlines my commitment to providing the best possible care that I can, which in turn must be based on ongoing professional development, diligence and a focus on the patient’s needs.
The second conclusion I draw from my reflective processes is that while a reflective cycle can guide reflection, it cannot provide the answers to the questions that are raised. The value of reflection lies in the ability to take those questions, answer them honestly, and to seek out the knowledge and information required to explore those answers in relation to practice as well as in relation to the self. As with my previous point, the process of professional development has led me to understand my role as one aspect of a greater whole, a complex network of professionals and roles, where roles and activities may overlap, but where the competence of each individual contributes to the whole, and where, if one component is missing, or lacking in some way, the whole is affected. If my communication skills are insufficient, this affects the work of others, their ability to meet patients’s needs, which impacts, sometimes significantly, on patient wellbeing and the patient experience. For children, who are perhaps the most vulnerable patient group, the impact is likely to be greatest. Therefore, reflection is no mere academic exercise, it is the means by which I can remind myself of my place within this network, and value my contributions whilst also appreciating the responsibility of my future position. Again, this is a motivation to provide excellence in practice, to ensure the continued quality of the whole.
While the development of nursing expertise is viewed as a foundation to professionalism (Hodkinson and Issit, 2004), I would argue that expertise is still poorly defined because in nursing it is very complex, and the intersections of various domains of practice are blurred, such that, for example, clinical skills are inseparable from other skills. Personal effectiveness in the nursing role may be more important in terms of professional development (Hodkinson and Isset, 2004). There are implications of this, however, for my role as a newly qualified staff nurse, because the change in expectations (on my own part and on others’), may lead to challenging transitions and some degree of reality shock (Evans, 2001). My reflections here have identified the fact that the socio-occupational integration into my qualified role is probably the most problematic (Evans, 2001). However, it is apparent that having engaged in a good degree of reflective practice throughout my training, I have developed the skills to be able to analyse and reflect upon experiences and situations, and to take this reflection further, by applying theory and evidence to my own practice. This requires not only a great degree of professionalism, but a commitment to ongoing professional development, preparing myself for the transition (Yonge, 2002), and continuing to view my working life as a continual process of learning and development.
References
Agnew, T (2005) Words of wisdom. Nursing Standard 20(6),pp24-26
Amos, D. (2001) An evaluation of staff nurse role transition. Nursing Standard 16 (3) 36-41
Andrews, M., Gidman, J. and Humphreys, A. (1998) Reflection: does it enhance professional nursing practice?. British Journal of Nursing 7(7) 413-7.
Ashworth, P. and Saxton, J. (1990).On competence. Journal of Further and Higher Education, 14, 3-25.
Bath, J.B., & Blais, K. (1993). Learning style as a predictor of drug dosage calculation ability. Nursing Educator 18(1), 33-36.
Beaney, A.M., Black, A., Dobson, C.R. et al (2005) Development and application of a ris
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gibbs reflective cycle"
Gibbs' Reflective Cycle was developed by Graham Gibbs in 1988 to give structure to learning from experiences. It offers a framework for examining experiences, and given its cyclic nature lends itself particularly well to repeated experiences, allowing you to learn and plan from things that either went well or didn’t go well. It covers 6 stages.
Related Articles