
Evaluation of gender variation in health awareness of Adolescent age groups in rural India
Introduction
World Health Organization (WHO) defines adolescence as the period between 10 and 19 years of age. During this period, they have to face a lot of changes which may include physical, mental, emotional or psychological changes. Yet they are the once whose health is neglected the most, especially that of female adolescent group. [1]
Health awareness not only includes the awareness for infections, diseases or disorders but also health related topics like physiological changes, psychological changes, hormonal changes, importance of exercise to stay fit, time for entertainment to stay active and happy etc. Adolescents in rural areas are often devoid of health care facilities and tends to fall sick more often. Both genders faces different types of problems. They even get addicted to un-healthy activities due to lack of awareness and peer pressure. Government of India has implemented many schemes for the spread of health awareness, but due to unknown reasons, it is not yet uniform among both the genders.
If they are aware of health issues surrounding them, they can fight or prevent them and can improve their lives. Female’s health has been always neglected in rural India and now as to be prioritised because not only they support family by sharing the economic burden but they also take care of the entire family. In order to share all responsibilities both males and females have to be fit and that should start from the very beginning, right after birth.
With implementation of new schemes and involvement of latest technology like internet; health awareness is improving[2] The teachers also teach them the benefits of health exercise and the requirement of time for recreational activities so that they can live a happy life.
Various studies and survey have been conducted before but none showed the difference of health awareness between males and females of adolescent group. So we conducted this study to access the gender variation in health awareness in adolescent age group [15-19 years].
Their answers to the questionnaire can help us to understand the awareness of health in rural areas and we could bring further changes or implement new plans for spreading health awareness especially if one of the gender is lacking behind in one area.
Material and Methods
The present study was conducted as a cross-sectional study in September, 2014 at a local school in Nhava village, Raigad District in Maharashtra State, India. A well-structured questionnaire was distributed randomly to 102 high school students which included 60 males and 42 females between 15 to 19 to evaluate gender variation in health awareness and attitude towards awareness of side effects of tobacco consumption leading to oral or lung cancer, Sexually Transmitted Diseases (STD) and its transmission route, reaction on stress situations, knowledge of body mass index and ill effects of being malnourished, importance of having breakfast and in between meals with time for exercise and recreational activities, evaluating depression by asking mood changes. Their family type, number of members and average family income, per capita income were also found out. They were asked if they suffered from any other disorders or diseases.
The required official permission to select and collect the relevant data from selected subjects was solicited and obtained from the Principal of the respective school. There were 13 questions and the questionnaire was collected on the spot from participants after explaining them the importance of study and obtaining their oral consent. Writing names on the form was optional and was informed that their identity will be kept hidden in all ways possible if they chose to write their names. The survey was carried out in their school timings and free periods.
Inclusion Criteria
- All Students between 15-19 years
Exclusion Criteria
- Students out of target i.e. above 20 years of age and below 15 years
- Who did not wanted to be a part of the survey
Statistical analysis
The data were entered into the computer (Microsoft Office, Excel) and were subjected to statistical analysis using the statistical package SPSS version 19.
Results
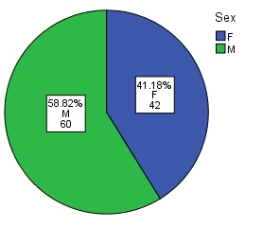
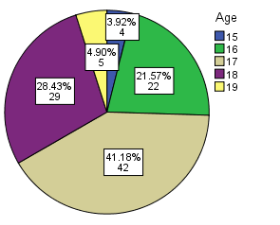
In the present study, we got 102 samples out of which 60 were males and 42 were females having 41.18 percentage of females and 58.82% of males. Also the ages ranged from 15-19. Most number of the students were in 17th year.
- Breakfast Everyday & In between meals 2-3 hours (Table 1)
Here we noticed that only 69% Females said that they were able to have breakfast as compared to 81.7% Males. Values are given in Table 1. n=Number, %= percentage
|
Sex |
Breakfast everyday & In between meals every 2-3 hours |
||||||||
|
Yes |
Not able to have |
Total |
|||||||
|
N |
% |
N |
% |
n |
% |
||||
|
F |
29 |
69.0 |
13 |
31.0 |
42 |
100.0 |
|||
|
M |
49 |
81.7 |
11 |
18.3 |
60 |
100.0 |
|||
|
Total |
78 |
76.5 |
24 |
23.5 |
102 |
100.0 |
|||
Table 1
- Time for Exercise & Recreation ( Table 2)
We noticed that 57.1% females here just said that they are able to do exercise and spare some time for recreation as compared to 80% approval from the males regarding the same.
|
Sex |
Time for exercise and recreation |
||||||||
|
Yes |
No |
Total |
|||||||
|
N |
% |
n |
% |
n |
% |
||||
|
F |
24 |
57.1 |
18 |
42.9 |
42 |
100.0 |
|||
|
M |
48 |
80.0 |
12 |
20.0 |
60 |
100.0 |
|||
|
Total |
72 |
70.6 |
30 |
29.4 |
102 |
100.0 |
|||
(Table 2)
- Consume Tobacco in any form or any other substance abuse (Table 3)
It is interesting to see that only 5 males used to consume tobacco in cigarettes form which is 4.90%. Females denied taking any tobacco in any form. The values are depicted in table 3
|
Sex |
Consume tobacco in any form or any other substance abuse |
||||||||
|
Yes |
No |
Total |
|||||||
|
N |
% |
n |
% |
n |
% |
||||
|
F |
0 |
.0 |
42 |
100.0 |
42 |
100.0 |
|||
|
M |
5 |
8.3 |
55 |
91.7 |
60 |
100.0 |
|||
|
Total |
5 |
4.90 |
97 |
85.10 |
102 |
100.0 |
|||
Table 3
- Awareness of the side effects of taking Tobacco in any form (Table 4)
Here we noticed that Females are more aware of the side effects of taking tobacco. Their awareness rate is 95.2% as compared to 78.3% of Males. The values are depicted in table 4.
|
Sex |
Awareness of side effects regarding tobacco & Substance abuse |
||||||||
|
Yes (Aware) |
No |
Total |
|||||||
|
N |
% |
n |
% |
n |
% |
||||
|
F |
40 |
95.2 |
2 |
4.8 |
42 |
100.0 |
|||
|
M |
47 |
78.3 |
13 |
21.7 |
60 |
100.0 |
|||
|
Total |
87 |
85.3 |
15 |
14.7 |
102 |
100.0 |
|||
Table 4
- Awareness of STD’s & at least one route of spread (Table 5)
Mostly everyone knows about STD and its of route of spread. More details are depicted in table 5.
|
Sex |
Awareness of STD |
||||||||
|
Yes |
No |
Total |
|||||||
|
N |
% |
n |
% |
n |
% |
||||
|
F |
42 |
100.0 |
0 |
.0 |
42 |
100.0 |
|||
|
M |
58 |
98.04 |
2 |
1.96 |
60 |
100.0 |
|||
|
Total |
100 |
98.04 |
2 |
1.96 |
102 |
100.0 |
|||
Table 5
- BMI Status & Awareness to ill effects of malnourishment (Table 6-8)
BMI of the study subject was calculated by using the formula weight (kg)/ height2 (m2). For grading proposed criteria of BMI for Asians (Choo V 2002) and CDC (2010) was adopted.
We noticed that females tend to be more underweight as compared to males. Males being more prone to obesity at this age. The mean BMI for females was 20.41
|
Sex |
BMI Status |
||||||||||||||
|
Normal |
Obese |
Over Weight |
Underweight |
Total |
|||||||||||
|
N |
% |
N |
% |
n |
% |
n |
% |
n |
% |
||||||
|
F |
29 |
69.0 |
0 |
.0 |
1 |
2.4 |
12 |
28.6 |
42 |
100.0 |
|||||
|
M |
42 |
70.0 |
1 |
1.7 |
2 |
3.3 |
15 |
25.0 |
60 |
100.0 |
|||||
|
Total |
71 |
69.6 |
1 |
0.98 |
3 |
2.94 |
27 |
26.47 |
102 |
100.0 |
|||||
Table 6
|
Sex |
Statistic |
Std. Error |
|||
|
BMI |
F |
Mean |
20.417341 |
.4574878 |
|
|
95% Confidence Interval for Mean |
Lower Bound |
19.493425 |
|||
|
Upper Bound |
21.341256 |
||||
|
Std. Deviation |
2.9648599 |
||||
|
Minimum |
15.0597 |
||||
|
Maximum |
26.3146 |
||||
|
M |
Mean |
21.016615 |
.4933969 |
||
|
95% Confidence Interval for Mean |
Lower Bound |
20.029330 |
|||
|
Upper Bound |
22.003900 |
||||
|
Std. Deviation |
3.8218361 |
||||
|
Minimum |
16.0231 |
||||
|
Maximum |
40.4281 |
||||
|
Table 7 |
|||||
BMI values are depicted in Table 7
We also asked them if they knew the ill-effects of being malnourished? Almost 90% males knew the ill effects. Whereas 78.6% Females knew about the ill effects. The details are in table 8.
|
Sex |
Aware of ill-effects of being malnourished? |
||||||||
|
Yes |
No |
Total |
|||||||
|
N |
% |
n |
% |
N |
% |
||||
|
F |
33 |
78.6 |
9 |
21.4 |
42 |
100 |
|||
|
M |
54 |
90.0 |
6 |
10.0 |
60 |
100 |
|||
|
Total |
87 |
85.29 |
15 |
14.70 |
102 |
100 |
|||
Table 8
- Mood & Study duration in a day (Table 9 & 10)
We also asked whether they stay happy & content always or unhappy and grumpy or scared or always angry. Most of them answered that they stay happy always. Most also mentioned that they study for 1-2 hours daily.
|
Sex |
Mood |
||||||||||||||
|
Always Happy & Content |
Always unhappy |
Always Scared |
Alway angry |
Total |
|||||||||||
|
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
||||||
|
F |
37 |
88.1 |
4 |
9.5 |
1 |
2.4 |
0 |
.0 |
42 |
100.0 |
|||||
|
M |
55 |
91.7 |
2 |
3.3 |
2 |
3.3 |
1 |
1.7 |
60 |
100.0 |
|||||
|
Total |
92 |
90.19 |
6 |
5.88 |
3 |
2.94 |
1 |
.98 |
102 |
100.0 |
|||||
Table 9
|
Sex |
Average hours of study per day |
|||||||||||
|
1-2 hours |
2-4 hours |
4-6 hours |
Total |
|||||||||
|
n |
% |
n |
% |
n |
% |
n |
% |
|||||
|
F |
25 |
59.5% |
14 |
33.3% |
3 |
7.1% |
42 |
100.0% |
||||
|
M |
41 |
68.3% |
17 |
28.3% |
2 |
3.3% |
60 |
100.0% |
||||
|
Total |
66 |
64.70% |
31 |
30.39% |
5 |
4.90% |
102 |
100.0% |
||||
Table 10
- Reaction on Stress or Depression (Table 11)
We noticed that almost half of them prefer to talk to their friends when they are depressed. Few females do cry or starve as well.
|
Sex |
Reaction on being stressed / depression |
||||||||||||||
|
Be alone / lock yourself |
Cry / Starve |
Call your friend |
Talk to your elders |
Total |
|||||||||||
|
n |
% |
n |
% |
N |
% |
n |
% |
n |
% |
||||||
|
F |
8 |
19.0 |
7 |
16.7 |
18 |
42.9 |
9 |
21.4 |
42 |
100.0% |
|||||
|
M |
15 |
25.0 |
5 |
8.3 |
28 |
46.7 |
12 |
20.0 |
60 |
100.0% |
|||||
|
Total |
23 |
22.54 |
12 |
11.76 |
46 |
45.09 |
21 |
20.58 |
102 |
100.0% |
|||||
Table 11
We also asked for any other diseases or disorder which they may be suffering from. 2 of males said that they are suffering from Diabetes and 1 female had ulcers. We also took family history which included number of family members, earning members, total family income per month and level of education.
Discussion
Adolescents are the future of the country. As they reach puberty, they face a lot of changes in many ways which includes physiological, hormonal, emotional and mental. Females tends to receive more challenges because of the physiological and hormonal changes occurring with the start of their puberty. [3] With the rise of menstrual cycle they often tend to get more depressed before getting adjusting to it.
BMI Importance & Awareness of malnourishment
Females may face malnourishment due to male children being given priority to eat first [4] or may be due to body weight consciousness leading to disorders like bullaemia or Anorexia nervosa or depression. [5]
Dr. Shah had conducted a study on nutrional assessment of adolescent girls in karamsad and had found out that only 8% girls were overweight while 63.2% were of normal weight and 28.5% were underweight. While 23.4% boys were overweight and only 21.2 % were underweight.[6]
The present study showed that 28.6% females were underweight as compared to 25% males. 2.4% females were overweight whereas we did not find any obese female during the study. 4% males were above normal stage which includes overweight and obese. Almost 90% males knew the ill effects. Whereas 78.6% Females knew about the ill effects.
STD Awarness & its route of transmission
In later years of adolescent age, teenagers especially males tends to get physically attracted and intimated with the opposite sex and the risk of contacting STD’s rises if proper protection not used.7] Dr. Kotecha had conducted two studies in urban and rural areas respectively, amongst school going students regarding reproductive health awareness and found out that in both rural and urban areas; about one-third of the boys and one-fourth of the girls knew about contraception. Two-thirds of boys and girls had information of HIV/AIDS, and about half of them correctly knew various modes of transmission of HIV in both urban and rural areas. Majority of the adolescent were even ready to visit the Adolescent Friendly clinic if there was any in near-by areas. [8,9]
The awareness regarding modes of transmission of HIV/AIDS was found to be higher among boys as compared to girls which contradicts the present study. [10] The present study showed that all females knew about STD’s and at least one route of spread as compared to 98.04% males. The contradiction might be due to improvement of health awareness in recent times.
Tobacco Consumption
Along with rise in STD’s prevalence and incidence there is a rise in increase of cigarette smoking among adolescent age [11] andstudents are vulnerable to tobacco addiction, especially males.[12]This can have harmful effect. A study conducted in state of Gujarat, India, showed that there has been increasing trend of smoking cigarettes at younger which is a matter of great concern13]. Early use of tobacco smoking may lead to many harmful effects like hypertension, lung cancer and may even lead to end stage organ in later years of life[14].
A study conducted by Sharma Et Al showed 18.4% males have tried cigarettes or bidis at least once in life time compared to 11% females in adolescent age group. Tobacco use was much higher among the adolescent aged 16-19 group than those in the age group of 14-15 years. Tobacco use was appreciably higher among the males (23.8%) than the females adolescent age group (14.9%), (P=0.016).The prevalence rate of current smoking is 7.1%[15].
The present study showed that 4.9% males has consumed tobacco in any form in a rural area which leads to a conclusion that the tobacco consumption might be at a larger scale in urban areas. All females denied taking tobacco in form. It also noticed that females are more aware of the side effects of taking tobacco. Their awareness rate was 95.2% as compared to 78.3% of Males.
Also adolescents are at increased risk of getting stress related depression. [16]They are easily influenced by changes around them which affects their biological, emotional, cognitive, and social functions. Unhealthy and anti-social behaviours are manufactured in these years but if stopped, can be moulded back or may change permanently. [17]These anti-social changes are common in males as compared to females
Conclusion:
There are many differences in health awareness between males and females of the adolescent age group. We need to decrease the bridge between them and for that we need to change some of our health policies. In some areas females have better health awareness like awareness in STD spread and side effects of taking tobacco in any form, whereas males have better knowledge in understanding the importance of taking proper breakfast and in taking some time off for entertainment. Along with that they also know the ill effects of malnourishment. If we need our youth to progress at a faster rate, we need them to be healthy at mind, body and free from diseases. For that, we need to inculcate health awareness in both genders and should decrease the bridge between the awareness.
Limitation & future perspective:
Sample size of study was small due to limited number of students in the school. In future, we want to study on more than 500 students of multi-schools in more than 5 districts involving rural areas.
References
- Mahajan P, Sharma N. Awareness level of Adolescent Girls Regarding HIV/AIDS (A comparative study of rural and urban areas of Jammu) J Hum Ecol. 2004;17:313-4.
- Gray NJ, Klein JD. Adolescents and the internet: health and sexuality information. Curr Opin Obstet Gynecol. 2006;18(5):519-24. doi: 10.1097/01.gco.0000242954.32867.76.
- Goldenring J. A Review provided by VeriMed Healthcare Network, Medline plus. 2004
- Borooah VK. Gender bias among children in India in their diet and immunization against disease. Soc Sci Med. 2004;59:1719-31.
- Reijone JH, Pratt HD, Patel DR, Greydanus DE. Eating disorders in the adolescent population: An overview. J Adolesc Res. 2003;18:209-22.
- Hasmukh, S., Wasim, S., & Singh, S. K. (2012). Are Indian adolescent girl students more conscious about their body image than their colleague boys? National Journal of Community Medicine, 3(2), 344-347.
- Weinstock H, Berman S, Cates W. Sexually transmitted diseases in American youth: Incidence and prevalence estimates. Perspect Sex Reprod Health 2004366-10.10
- Kotecha PV, Patel SV, Mazumdar VS, et al. Reproductive health awareness among urban school going adolescents in Vadodara city. Indian Journal of Psychiatry. 2012;54(4):344-348. doi:10.4103/0019-5545.104821.
- Kotecha PV, Patel S, Baxi RK, et al. Reproductive health awareness among rural school going adolescents of Vadodara district. Indian Journal of Sexually Transmitted Diseases. 2009;30(2):94-99. doi:10.4103/0253-7184.62765.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gender"
Gender is the range of characteristics pertaining to, and differentiating between, femininity and masculinity. Depending on the context, these characteristics may include biological sex, sex-based social structures, or gender identity.
Related Articles
