
Introduction.
Professional development and up to date practice is a requirement of the nursing profession. Reflection is a vital component of this (Gustafson and Fagerberg, 2004) and allows nurses to critically and actively evaluate their practice in the light of current research and their own learning. Reflection has been defined as a process of describing experiences and then using reflection as a basis from which to ask questions about practice (Bowden, 2003). The NMC (2004) states that nurses should use professional standards of practice to self-assess performance. This essay evaluates my own learning in relation to the NMC Standards through the use of a reflective cycle by Gibbs (1998) (see Appendix). The focus of the reflection is Inter-professional (IP) working. IP is a fundamental component of education programmes for Nursing, Midwifery and Allied Health Professions (Pollard et al, 2004). The NMC (2004) states in the standards of proficiency for entry to the register that student nurses should:
- “consult other health care professionals when individual or group needs fall outside the scope of nursing practice.” (p26).
- “utilise a range of effective and appropriate communication and engagement skills” (p 27).
- “seek specialist/expert advice as appropriate.” (p28)
- “establish and maintain collaborative working relationships with members of the health and social care team and others.” (p32)
- “participate with members of the health and social care team in decision-making concerning patients and clients.” (p32)
- “review and evaluate care with members of the health and social care team and others.” (p32)
Description: What Happened.
In providing care for clients allocated to me on the general medical ward, I engaged with the case of Mrs B, who had been admitted seven days previously from a nursing home with dehydration and confusion. Mrs B was registered blind, and required full nursing care which was delivered according to a care plan. Having been treated with IV fluids and encouraged with diet and oral fluids, she had made a good recovery and my role was to implement a discharge planning process with her, so that she could return to the nursing home.
In order to assess her discharge needs, I consulted occupational therapy colleagues, dieticians, medical colleagues and social work colleagues to ensure that her needs would be met in her home environment. I also attended the ward rounds with the medical consultant and his team, to gain the expert advice needed to ensure all Mrs B’s needs were met and that she was well enough for discharge. In collaboration with other nursing colleagues and the occupational therapist, dietician and social worker, I reviewed the care plan, carried out a thorough reassessment and evaluation of Mrs B’s condition, medication and ongoing care needs, and drew up a comprehensive discharge plan, including communication to the receiving nursing home. I also discussed all of her needs with Mrs B, and her family, and ensured their input was included into the discharge plan.
Feelings
The sense of responsibility attached to discharge planning is considerable, and I was aware that I needed to ensure all Mrs B’s needs had been addressed. I felt uncomfortable in some of my interactions with other professionals, and frustrated at times with communication issues.
Evaluation
I felt confident in care planning and evaluation, having had ample opportunities to develop these skills over my training, but was also aware of the scrutiny of colleagues. This kind of scrutiny was double-edged, in that I felt uncomfortable to be the subject of scrutiny but that it also helped me to focus on the highest standards of care. It was difficult sometimes to ensure timely communication with these colleagues, and the responsibility for ensuring collaborative working and good communication was also somewhat stressful.
Analysis
At this stage of my training, I was very aware of requirements that I meet standards of competency related to the nursing role. This led to an initial reconsideration of what competency actually is. For example, competency has been described as being able to complete tasks (Gonczi 1993), but professional competence is much more than this. In this case, the ability to complete single tasks was evident in my ability to plan and manage care. Identifying individual nursing tasks in relation to Mrs B was a part of this process, and the process contains in-built mechanisms of evaluation which, if applied objectively, allow the nurse to ‘tick off’ tasks as achieved or in progress. But the complexity of care planning does not led itself to a simple task-based approach, and it is here that the greatest challenge to competence can be identified. The holistic approach to nursing requires the nurse work in a collaborative, inter-professional manner. In particular, it is important to take into account the context of nursing care and presence and contribution of others, including their effect on performance (Ashworth and Saxton, 1990; Field, 1991; Collins, 1991).
The NSF for Older People demands the provision of care services which are based around the needs of older people and their carers (DOH, 2001). In order to meet these needs, there is a need to employ “an integrated approach to service provision… regardless of professional or organisational boundaries.” (DOH, 2001, p9.) Thus IP working can be seen to be fundamental to the process of discharge planning for Mrs B. One of the challenges for my practice was to identify all the other professionals who might need to be engaged in this process. Some of these were obvious, such as the medical team, other nurses, and the dietician, who already played a fundamental role in her care management and implementation. The other professionals involved were not as obvious, and I had to consult with senior nurses to identify where other professional colleagues might be important in discharge planning.
There were also other challenges in this process, in engaging with other professionals and carrying out individualised discharge planning. The NSF for Older People recognises that this has been a problem in the past, acknowledging that organisational structures have hitherto had the effect of impeding the provision of individualised care management packages (DOH, 2001.) One of the difficulties I reflected upon was the conflicting demands of such an individualised process which formed only one of my many nursing duties in a busy medical ward environment. And the sense of achievement I felt in taking such responsible role was not always reflected in the ways in which other colleagues interacted with me.
Discussion with other nursing colleagues, and some exploration of the theoretical and research literature on this subject identified that this is no new experience for nurses engaged in IP working. Research seems to indicate that medical hegemony leads to the pivotal role of nurses in IP working being largely unacknowledged, which can affect the development of collaborative care practices (Coombs and Ersser, 2004). However, a new awareness of this issue made me more confident and proactive in engaging with other professionals, which led to a negotiation of sorts, during the communication process, between my role and some of their perceptions of my role and position in the institutional hierarchy. There were definite lessons to be learned from this in particular. Adapting modes of communication, paying attention to communication, and formalising communication through detailed record keeping all supported this process.
I also learned how vital the nursing role is in inter-professional, client-centred working, if the highest standards of care are to be consistently achieved and maintained for every client. Some authors argue that nurses, as the primary care contact for the majority of patients, should seek to distinguish and celebrate their practice as professionally discrete from that of others because of their intimate and sustained knowledge of their clients (Price, 2006). This is a really important point, and one which allows me to take my experience forward into future practice and build on my confidence in addressing challenging situations.
Conclusion
I felt that I ‘matured’ through this particular care incident and my own reflections upon it, coming to terms with a sometimes uncomfortable reality of persistent hierarchies, stereotypical beliefs and defensive protection of professional role boundaries. My own competence in achieving an excellent discharge process, engaging in communication despite considerable challenges, and ensuring individualised care in an IP context were all signposts of considerable achievement in my professional journey. However, I could also have perhaps worked more collaboratively with other colleagues, qualified nursing colleagues in particular, who might have been able to give me some advance warning of these issues and perhaps identified ways in which I could overcome them. Instead, I learned the hard way.
Action Plan
- Explore alternative strategies for inter-professional communication.
- Carry out further research into the challenges of IP working and its benefits.
- Explore ways to safely challenge rigid roles and hierarchies whilst still providing client-centred care.
- Seek out support from colleagues when challenging situations arise and build on this experience in future nursing practice.
- Carry out future cycles of reflection on similar clinical issues, and compare these to previous reflections to clearly signpost my own learning and development.
References
Ashworth, P. and Saxton, J. (1990).On competence. Journal of Further and Higher Education, 14, 3-25.
Bowden, S.D. (2003) Enhancing your professional nursing practice through critical reflection. Abu Dhabi Nurse Summer 28-31.
Collins, M. (1991). Adult education as vocation. London: Routledge.
Coombs, M. & Ersser, S.J. (2004) Medical hegemony in decision-making – a barrier to interdisciplinary working in intensive care? Journal of Advanced Nursing 46 (3) 245-252.
Department of Health, (2001) National Service Framework for Older People. Available from www.dh.gov.uk/publications accessed 22-3-07.
Field, J. (1991). Competency and pedagogy of labour. Studies in Education of Adults, 33(1), 41-52.
Gonczi, A. (1993). Competence and competencies: A global perspective. Paper presented at the First National Conference on Competencies in Nursing Adelaide: Australian Nursing Federation (SA Branch)
Gibbs, G. (1988) Learning by Doing. A Guide to Teaching and Learning Methods Further Education Unit, Oxford Polytechnic, Oxford
Gustafsson, C. and Fagerberg, I. (2004) Reflection: the way to professional development? Journal of Clinical Nursing 13 271-280.
Knight, P. (1995) Assessment for Learning in Higher Education London: Kogan Page.
Neary, M. (2000) Responsive assessment of clinical competence. Nursing Standard 15 (10) 35-40.
Nursing and Midwifery Council (2004) Code of Conduct Available from www.nmc-uk.org Accessed 30-4-07.
Pollard, K.C., Miers, M.E. & Gilchrist, M. (2004) Collaborative learning for collaborative working? Initial findings from a longitudinal study of health and social care students. Health and Social Care in the Community 12 (4) 346-358.
Price, B. (2006) Exploring person-centred care. Nursing Standard 20 (50) 49-56.
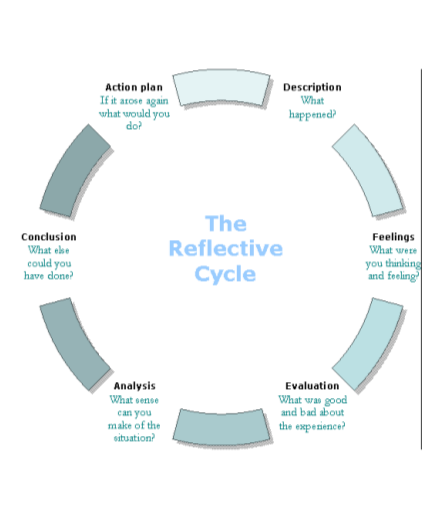
Appendix
Gibbs (1988) Cycle of Reflection
Cite This Work
To export a reference to this article please select a referencing style below: