A report was published in 1992 in The House of Commons regarding the provision of maternity services; it stated that ‘all hospitals make it their policy to make provision wherever possible for women to choose the position which they prefer for labour and birth with the option of a birthing pool where is practicable’ (House of Commons Health Committee 1992). Water immersion was officially accepted in the UK in 1993 following the publication of the Changing Childbirth report (Department of Heath 1993). This report recommended that a pool facility should be available in all UK maternity units; professional recognition came about when the Royal College of Midwives (RCM, 1994) and the United Kingdom Central Council for Nursing, Midwifery and Heath Visiting (UKCC 1994) published statements in 1994 which integrated the immersion in water during labour into the midwifes role. Water immersion is now incorporated in the UK Midwifery Rules and Standards (2004).
The current guidelines for labouring in water in Forth Valley are that the woman should be in established labour, determined as cervical dilation of a minimum of 4cm, be at least 37 weeks gestation, the presentation of the fetus should be cephalic and the fetal heart should be within normal parameters of 110 – 160 beats per minute, any liquor draining should be clear and no opiates should have been administered in the 4 hours proceeding entry to the pool (Paterson & Hamilton, 2009). The water temperature should be 37 degrees; this should be checked hourly together with the temperature of the woman to ensure that she is not pyrexial (NICE, 2007). The woman must also have an uncomplicated obstetric history. At present the facility to labour in water is present in Stirling Royal Infirmary however there is currently only 1 labour room with a pool. This means that only 1 woman can labour or give birth in water at a time. All woman are offered the option of a water birth at their booking visit however whether or not they will be able to labour or give birth in water will be dependant on the pool being vacant when they present in labour.
The benefits of labouring in water are plentiful and is recommended in the NICE Guidelines for Intrapartum Care (2007); the buoyancy afforded by water allows the labouring woman to adopt comfortable positions easily and the water also provides a relaxing environment which assists pain relief due to the release of natural endorphins (Medforth et all, 2007). When a woman feels relaxed oxytocin is released which is required for successful contraction of the uterus and progress in labour; the reduction in feelings of stress will inhibit the production of adrenaline which if produced will hinder oxytocin production therefore slowing the progress of labour. Evidence suggests that the use of water in the first stage of labour empowers woman with an increased feeling of control over the situation she is experiencing (Hall & Holloway, 1998) it also shown that as the women’s perception of pain is reduced the need for epidural analgesia is lessened (Eberhard et all, 2005) as is the need for augmentation by syntocinon (Cluett et all, 2004). Studies have shown that woman who give birth in the water have a reduced incidence of perineal trauma (Garland and Jones, 2000). This has been further supported by a clinical audit carried out in Corbar birth Centre, Baxter (2006) found that of 229 pool births 38% of woman had an intact perineum, 32% had a first degree tear, 29% sustained a second degree tear and only 1 woman suffered a third degree tear however this was the result of an accelerated second stage labour and the birth of a baby weighing in excess of 4.5 kg. The audit also showed that women who laboured in the pool but did not give birth had a reduced incidence of perineal trauma. Of the 75 woman 32% had a first degree tear, 31% had a second degree tear and again 1 woman suffered a third degree tear however 31% did require an episiotomy. It has been suggested that it is the atmosphere achieved that results in the positive experiences and outcomes for the woman who choose to use the pool through the continuous one to one care of the midwife, the woman centred approach to childbirth thus normalising the birthing experience.
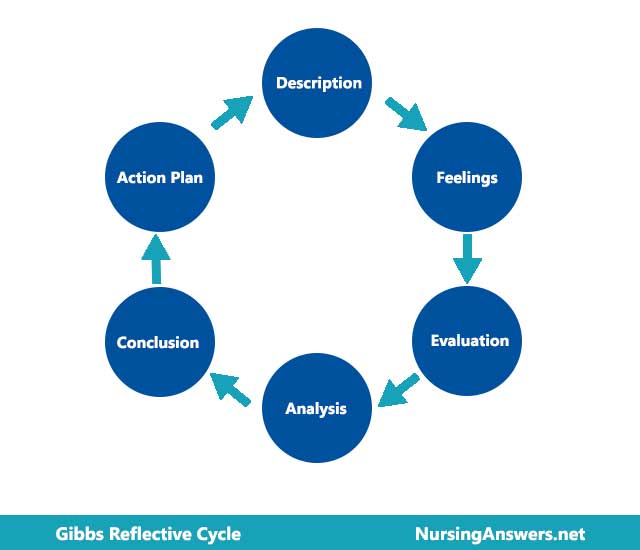
The student will now reflect on her experience of a water birth using Gibbs reflective cycle. “I came onto an early shift on the 27 February and my mentor and I were allocated the care of a woman in established labour who had decided to labour in water. We entered the room where we were introduced to Sarah and her partner John. Sarah was a primigravida with an uncomplicated obstetric history and had been well throughout her pregnancy, her body mass index of 22 was within normal parameters. The staff midwife we were taking over from gave a handover, detailing what had happened since Sarah had arrived in the ward; Sarah’s labour had commenced spontaneously at home at 41 weeks and 8 days gestation, at 2am that morning she had arrived in maternity triage for assessment; at 5am she had been transferred to the labour ward, at this time she was 3cm dilated and struggling to cope with the pain. Sarah wasn’t keen to use pain relief other than entonox and the midwife providing her care had read in her maternity notes that in the past few weeks that she had been considering labouring in water, therefore she suggested Sarah could try using the pool for pain relief; both the advantages and disadvantages were fully explained to Sarah and she was advised that if her own or the fetal condition deteriorated then she would be asked to leave the pool. Before going into the water Sarah’s membranes had been ruptured artificially and following the procedure she was 5cm dilated at 6am, therefore she was in active labour and suitable for labouring in water.
Upon taking over Sarah’s care a set of baseline observations were carried out by myself, including a blood pressure, temperature, pulse and urinalysis. The fetal heart was heard regularly at 120 – 130 beats per minute (NICE, 2007). I also checked the water temperature which was 37 degrees. All observations were satisfactory; these were noted both on the partogram as well as the labour notes. Observations of temperature and pulse were carried out hourly, the water temperature was checked regularly and Sarah’s blood pressure would be checked 4 hourly. The fetal heart was auscultated intermittently using a waterproof Doppler ultrasound. Sarah was using the entonox in the pool and although she was still finding the contractions painful she was coping well. Encouragement was given to Sarah during this time, reassuring her that she was doing fantastically and guidance on using the entonox effectively. The atmosphere in the room was relaxed and calm, John was also giving encouragement. At around 8.30 am, 1 hour after taking over Sarah’s care, she said reported that she was experiencing a burning sensation and was feeling the urge to push. The staff midwife put a mirror into the pool and the vertex was found to be visible at this stage. As per the protocol (2009) Sarah was advised to push when she felt the urge but to remember not to raise her bottom out of the water. Encouragement was given to Sarah when she was pushing, but no direction was given as directed pushing is not recommended for birth in water (Baston & Hall, 2009). The baby’s head was delivered approximated 20 minutes later however the baby’s chin had not been seen as yet. The staff midwife put a hand into the pool to ensure that the chin was free and it was. A live female was delivered with the next contraction and was guided through Sarah’s legs as she was in a kneeling position and brought up to her chest.
The third stage of labour, the delivery of the placenta, was carried out on a Bradbury mattress as the protocol states that the placenta cannot be delivered in the pool (Paterson & Hamilton, 2009). This is due the difficulty in assessing the estimated blood loss in water. Syntometrine was administered intra muscularly by the staff midwife and the placenta was delivered by controlled cord traction approximately 30 minutes after the birth of the baby. Sarah had advised that she would like the cord to stop pulsating before it was cut and clamped therefore Sarah had remained in the water until this had occurred. Sarah had a 2nd degree tear following the delivery and although it was not actively bleeding it was sutured by the staff midwife approximated 1 hour post delivery as is recommended in the guidelines (NHS QIS, 2008).
The labour and birth were a beautiful and memorable experience as although it was evident that Sarah was in pain during the labour she was focused on birthing her baby. I felt very satisfied with the delivery as I felt Sarah had received the support and encouragement to have the experience of birth that she had strived for. The delivery underwater is amazing, I felt completely overwhelmed with how natural giving birth in water is as I had never experienced a water birth first hand. When reflecting on the experience I realised that upon taking over Sarah’s care I had felt slightly nervous about how ‘hands off’ a water birth is. The midwife is expected to basically observe both the labour and birth with the exception of carrying out the routine observations, checking and maintaining the temperature of the water and keeping the water as clear as possible with the use of a sieve. Since this experience I feel that the next time I am caring for a woman labouring or birthing in water I will feel more confident as this is a natural and therapeutic method which increases the focus on normality in childbirth.’
The use of hydrotherapy has been encouraged as a method of analgesia for many years as a natural alternative to pharmacological pain relief (Jessiman & Bryer, 2000). Water provides a dual benefit, heat alleviates muscle spasm and as a result of this pain is reduced and weightlessness lessens the effects of gravity therefore relieving the strain on the pelvis. Sarah was able to adapt her position easily whilst in the pool and spent the majority of her labour in a kneeling position thus facilitating the decent of the fetus (Fraser & Cooper, 2009). The NMC (2007:3) states that ‘You must recognise and the respect the contribution that people make to their own care and well being’ therefore if a woman wishes to labour and give birth in water it is the midwives duty to support her in this choice. Sarah had all the information in order to make an informed choice and felt that she had contributed to the care she received thus enhancing her satisfaction with her experience of labour. Eckert et all (2001:84) concluded their randomised controlled trial with the outcome that woman who labour and give birth in water ‘appeared more satisfied with their experience’ as was the case with Sarah. As a midwife advocacy is an important element of the role and it is important that midwives are advocates for the woman in their care in that they empower them with the knowledge to make informed choices regarding the care they receive (Garland, 2000).
Although the use of water has been attributed to reduced perception of pain (Baxter, 2006) there is still insufficient evidence to support the use of water and studies have shown that there is no significant difference in the length of labour, blood loss or Apgar scores at birth (Cluett & Burns, 2009). There have also been concerns surrounding the conditions of the neonate born in water; yet as stated there has been no evidence found to support this. In fact Thoni and Moroder (2004:47) have stated that a water birth presented ‘no risk to the adaption of the neonate to extra-uterine life’. It is however vital that the woman is removed from the water should the maternal or fetal condition become compromised (Geissbuehler et all, 2004). There was also the question of maternal and fetal hyperthermia; the suggestion that the woman should decide the temperature of the water (Anderson, 2004) was rejected when NICE (2007) advised that the water temperature should be below 37.5 degrees. It has however been shown that entry into the pool in the latent first phase of labour can be detrimental to progress, Eriksson (1997) found that woman who entered the pool at this stage had increased augmentation of labour as well as increased requirement for epidural analgesia, hence the protocol in Forth Valley that woman should be in established labour prior to entering the pool (Paterson & Hamilton, 2009).
In conclusion, it appears that there is currently insufficient evidence to support the positive effects of hydrotherapy in labour and birth; its use has been proven to have a relaxing effect on labouring woman who have reported feeling more satisfied with their experience. Evidence suggests that labouring in water does not make a significant difference to the length of labour; however the fact that the women who choose this method of pain relief report increased fulfilment should not be over looked. Further research would provide an evidence base for best practice. At present only women with an uncomplicated obstetric history are permitted entry to a birthing pool and further research is required to enable women with a variety of obstetric backgrounds to utilise a pool confidently. The question of the environment attained through hydrotherapy has arisen; do women feel increased satisfaction due to the woman centred, one to one approach to care received? It seems that this is a significant factor, and one which great emphasis should be placed upon. The role of the midwife is to be ‘with women’; this requires the midwife to be an advocate for the women in her care, it also requires her to provide the women with information to make informed choices regarding their care and to treat every woman as an individual, with individual concerns and needs. If hydrotherapy provides a platform for a natural approach to childbirth then it is one that should be encouraged.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "gibbs reflective cycle"
Gibbs' Reflective Cycle was developed by Graham Gibbs in 1988 to give structure to learning from experiences. It offers a framework for examining experiences, and given its cyclic nature lends itself particularly well to repeated experiences, allowing you to learn and plan from things that either went well or didn’t go well. It covers 6 stages.
Related Articles