
Pediatric Case Report: Febrile Neutropenia in the background of B-ALL
Patient Details:
Age of patient: 4.5 years
Gender: Male
Date of Birth: 10/06/14
Date of presentation: 29/11/2018
Presenting Complaint:
The patient presented to the hospital on 29/11/2018 with a history of a temperature of 38.7 degrees Celsius, a head cold, runny nose and cough for one day on a background of B-ALL.
History of Presenting Complaint:
Prior to this admission, the patient presented to A&E at UCHG on 6/11/2018 with an intermittent fever which was recorded to be 37.9 degrees in addition to vomiting for one day. On examination, the patient’s throat was erythematous. The patient returned on 29/11/2018 with an intermittent fever of 38.7 degrees, head cold, runny nose, and cough on a background of B-ALL which was diagnosed September 7, 2017. This was the second fever the patient has had this year (2018).
Past Medical and Surgical History:
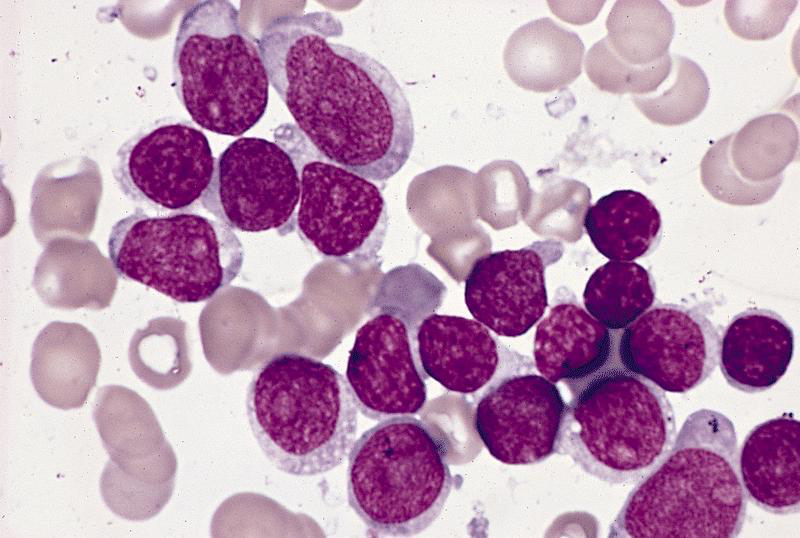
2017 – Patient was 3 years old. He presented to A&E with a 2-month history of ankle pain, lethargy and a cough that lasted two weeks. On examination, he was pale but alert. His cardiorespiratory exam was normal. He had hepatosplenomegaly and palpable left axillary and right groin lymph nodes. Blood counts showed a Hb of 6.9, platelets 128, LDH 270 and Uric Acid 287. A blood film was done which revealed >85% nucleated blast cells. The FBC results were then discussed with the hematology registrar.
December 20, 2017 – A bone marrow biopsy was performed which revealed 52.7 x10^9/L WBCs. A diagnosis of B-ALL was made. The patient and his family went for cytogenetic testing. This classified the patient as intermediate risk ALL. Patient’s parents were notified of the diagnosis. They were evidently distraught.
January 22, 2018 – The patient came in for a lumbar puncture under general anesthetic which was normal.
February 7, 2018 – Patient presented to the pediatric ambulatory care for IV cytarabine which was followed by a day’s duration of vomiting and retching. Received a PEWS score of 1. Standard labs were done (Hb 6.2). The patient then received a blood transfusion as per protocol.
March 5, 2018 – Patient came in for a lumbar puncture which revealed no abnormalities.
May 17, 2018 – Patient presented to the day ward for bloods. He had been having abdominal pain and an increase appetite of one day duration which was the most severe the previous night. He was not constipated and had been passing regular soft stools of normal color. It was determined that there were no red flags and may have been a minor case of gastritis. Patient was recommenced on Zantac 4mg/kg.
Medications and Allergies:
Dexamethasone 1mg PO bd until day 28 then taper to zero over 7 days
Cotrimoxazole 240 mgs PO bd on Saturdays and Sundays only as pneumocystis prophylaxis.
Morphine sulphate (10 mgs/5mls), 3 mgs 4-6 hrs prn for pain
Ondansetron 3 mgs every 8 hours prn for nausea
Movicol paed 1 sachet bd prn for constipation
No known drug allergies
Pregnancy and Birth History:
The patient was born as a singleton via Cesarean section due to a breech presentation. There were no complications during the surgery and the patient was brought to term. The patient’s mother had gestational diabetes, but was otherwise in good health throughout the pregnancy. There was no evidence of premature rupture of membranes, fevers, infections, or hypertension. There were no complications post-delivery. They did not require time in the intensive care unit. There were no feeding problems reported. Mother is G2 P2.
Developmental History:
The patient’s mother reported that he has met all developmental milestones so far. He is currently 4 and a half years of age with a normal weight and height.
Immunization History:
The patient has received all pertinent vaccines. They were all given at the normal ages of 2, 4, 6, 12, and 13 months of age. He was vaccinated through the HSE Primary Childhood Immunization Program (PCIP).
Family History:
The patient’s aunt passed away of breast cancer. The patient’s uncle passed away of lung cancer. The patient’s father has a diagnosis of heart flutter. There is no other relevant family history. No family history of diabetes, hypertension, congenital abnormalities, or immunodeficiencies.
Social History:
The patient resides in a home with his mother, father and older brother
Investigations:
Detailed examination for all possible sources of infection including the hickman line and noting any signs of systemic sepsis. The hickman like was in situ on the right side with signs of pus or purulent material and no signs of infection. Full ENT exam was unremarkable. Throat swab was taken and sent for microbiology.
29/11//18 Labs included a full blood count: WCC 2.1 Hb 9.3 Plt 90 Neut 0.2 CRP 24.2. A full blood count is important in this patient’s case as the chemotherapy regimen he has been receiving tends to lower his ANC (absolute neutrophil count). In addition, blood cultures must be sent from both the peripheral and central line. SMAC20 was included to check the status of his kidney and liver. A CRP was sent to unveil any signs of inflammation.
EXAMINATION:
Vital signs:
Respiratory Rate: 28
Respiratory effort: Normal
O2 T score: 0
SpO2: 97
Heart rate: 98
Capillary refill: Normal
Blood pressure: 83/44
AVPU: Normal
Temperature: 37.5 degrees Celsius
PEWS Score: 0
General
Patient was awake, sitting and standing upright, responsive, and alert. Color was slightly pale. There were no signs of respiratory distress. The patient appeared well nourished with no signs of cachexia.
Cardiovascular:
Heart sounds 1 and 2 were heard with no added sounds, murmurs, or gallops. No central or peripheral cyanosis. No clubbing was present.
Respiratory:
Vesicular breath sounds heart throughout with no wheezes or crepitations. Chest was clear. air entry bilaterally was normal. There was no shortness of breath, no use of accessory muscles and equal chest movement.
Gastrointestinal
GIT examination was normal with no hepatosplenomegaly felt. Abdomen was soft and nontender with no distension. No guarding present. No scars or hernias present. No masses felt. Bowel sounds were heard on examination.
ENT
No signs of infection in either ear. The tympanic membrane was visible bilaterally. Throat was no longer erythematous and tonsils were not enlarged. Tongue had a normal appearance and color. Nose was slightly runny. No facial or sinus tenderness. No cervical lymphadenopathy or tenderness.
Skin
Hickman line was in place on the right side. On examination, there was no erythema, rash or signs of infection present. The patient had normal mucous membranes, good skin turgor and no other signs of dehydration. No neurocutaneous lesions present on the patient.
Central Nervous System
No neurologic abnormalities were elicited. The upper limb, lower limb, cerebellar and cranial nerve exams unveiled no deficits. Normal tone, power, and movement of all limbs. Normal sensory responses. GCS 15/15.
Centiles:
SUMMARY:
The patient who is 4.5 years old presented to A&E at UCHG on Wednesday, 29/11/18 due to a temperature of 38.6 degrees in addition to a runny nose, head cold and cough of one day duration, on a background of B-ALL. Earlier this year, (6/11/2018) the patient presented to A&E with a temperature of 37.9 and vomiting for 1-day duration. The patient has a diagnosis of B-ALL, which was made on 20/12/17. A bone marrow biopsy confirmed the diagnosis and he was commenced on regimen B of UK-ALL 2011 clinical trial protocol. Since then, he has been seen regularly for chemotherapy and blood transfusions in Our Lady Children Hospital, Crumlin. His medical care is shared between UCHG and Crumlin. These chemotherapeutic drugs included asparginase, vincristine, daunorubicin, and dexamethasone. He has tolerated treatment well and has not developed any evidence of Tumor Lysis Syndrome or systemic sepsis. He was admitted to the pediatric ward where he was monitored, as this was his second fever this year. His labs on the day of his admission (29/11/2018) showed a White cell count of 2.1, a neutrophil count of 0.2 and a CRP of 24.2. This patient’s neutrophils have consistently been low since beginning chemotherapy.
Vitals upon admission were all normal except a slight elevation in temperature of 37.5 degrees. On general inspection, the patient was awake and alert. A full examination was conducted which revealed no abnormalities other than a runny nose and congestion. Normal centiles?
ASSESSMENT:
The patient presented with signs of an upper respiratory tract infection as well as a fever in the background of B-ALL. The patient has been on chemotherapy, which has reduced his white cell counts. This information points to a working diagnosis of febrile neutropenia. Due to the decreased white cell counts, his body no longer has the capacity to fight off opportunistic pathogens it may encounter. The patient had a fever and symptoms of an upper respiratory tract infection. In the FBC taken, the patient’s white blood cell count was 2.1 on and a (ANC) neutrophil count of 0.2 on 29/11/18. His temperature has risen to 38.6 the previous evening. This fits the criteria for febrile neutropenia. OLCHC guidelines recommend that patients with a temperature above 38 degrees and an ANC < .5 x 109 / L should be treated immediately. This also applies when the patient has been treated for chemotherapy within the last 6 months and is showing signs and symptoms of fever and infection, even if they are not necessarily neutropenic.
Parental concerns and expectations:
The patient’s parents were counseled that if their son had a temperature above 38 degrees, to present to the hospital as soon as possible. They were fully equipped and prepared to be admitted to have a significant stay in the pediatric ward. They were very clued into the care of their son and they knew that the treatment regimen he was receiving could cause all sorts of infections. This was his second time presenting with a fever due to febrile neutropenia. They expected that after a course of antibiotics, their son would begin to feel better and the fever would come down. They were awaiting discharge and showed no signs of concern.
DIFFERENTIAL DIAGNOSES:
Tumor fever:
Drug fever:
Thromboembolism:
Management plan:
Follow up:
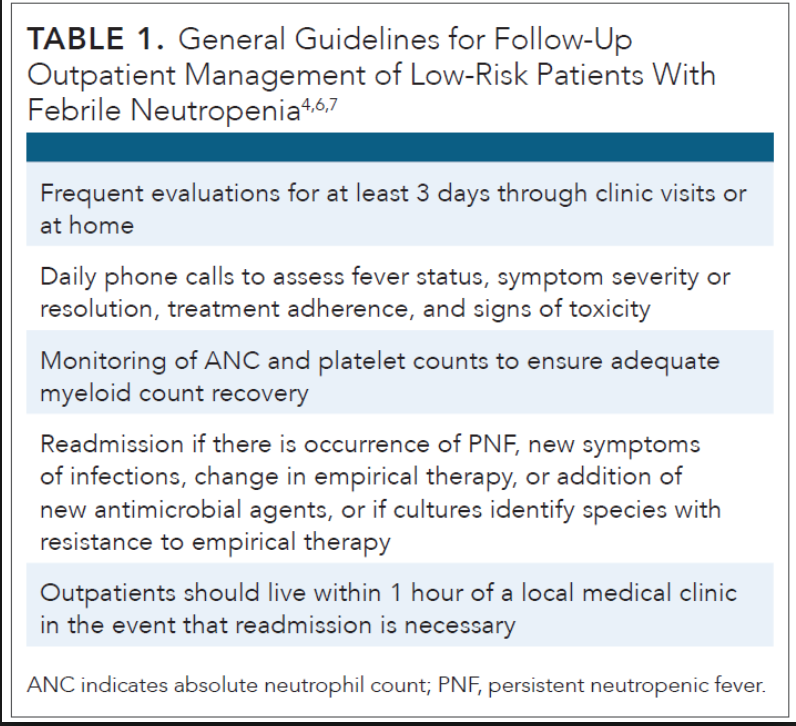
This patient’s follow up plan was to go to Dublin the following day after discharge to receive the beginning cycle of his maintenance phase and was due back in the day ward at regular intervals after that for standard treatment of bloods, transfusions etc. This patient should be closely monitored for similar presentation in the future. The American journal of Managed Care has guidelines for the follow up management of FN:
DISCUSSION:
REGIMEN B OF UK ALL 2011 CLINICAL TRIAL
The 2011 United Kingdom acute lymphoblastic leukemia trial (UK ALL 2011) is a phase III randomized trial for patients aged less than twenty-five years and greater than one year who have acute lymphoblastic leukemia (ALL) or lymphoblastic lymphoma. The patient, who was three years old when diagnosed with ALL, was an appropriate candidate for the trial and is currently in the fifth and final phase of regimen B of the UK ALL 2011 trial. The trial has a total of five phases, which together take just over three years for boys. The first phase is induction, where the patient receives intensive chemotherapy for five weeks. After the first phase, the patient is categorized into regimen A, B, or C. The patient’s regimen dictates the intensity of the ensuing treatment, where regimen A is the least intensive and regimen C is the longest and most intensive. The second phase is the consolidation phase, which consists of outpatient chemotherapy treatment for three, five, or ten weeks depending on which regimen the patient has been prescribed. Phase three is interim maintenance, where patients in regimens A and B are given less intensive oral chemotherapy treatment for about two months. Patients in regimen C will have a more intensive chemotherapy course. Phase four is delayed intensification, where the patient receives seven or eight weeks of intensive outpatient chemotherapy. Phase five is the maintenance phase, where the patient has infrequent outpatient chemotherapy for nearly three years for males. The two randomizations that make UKALL 2011 a randomized study occur first in the induction phase, and then the second randomization occurs in the maintenance phases. In the induction phase, there is variation between the intensity of the treatment and the length of time for which the patient is treated. Some patients are randomly assigned to dexamethasone at a higher dose for two weeks, while others are assigned to receive the traditional lower dose for four weeks. The second randomization has some patients receive a higher dose of methotrexate in the interim maintenance phase, and completely removes vincristine and dexamethasone from the phase 5 maintenance phase. (1)
Different drugs are used in different phases of the trial for chemotherapy. Table 1 (2) shows a comprehensive list of which drugs are used in each respective phase of the trial for patients in regimen B. Regimen C has all of the same drugs, however, each phase will use a larger and more diverse cocktail. Regimen A uses the same drugs; however, the number and amount of the drugs is smaller in each phase.
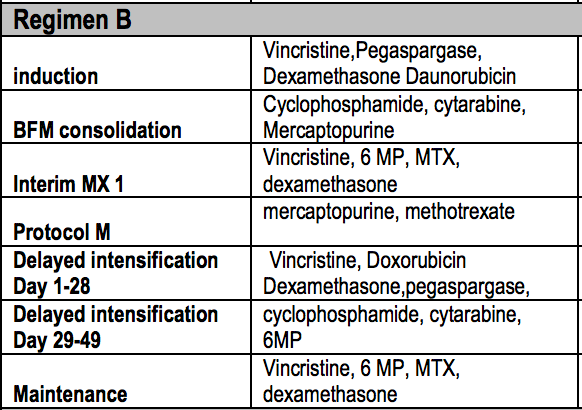
Table 1. (2) The five phases of the UKALL 2011 trial and
the drugs used for chemotherapy in each phase for a
patient in regimen B
FEBRILE NEUTROPENIA
Febrile neutropenia (FN), the occurrence of fever in a patient with a low number of neutrophils, is a recognized complication of myelosuppressive chemotherapy. FN is a life-threatening condition, and is the cause of 50-75% of deaths in acute leukemia patients who are administered chemotherapy (3). A patient is diagnosed with neutropenia when they have a neutrophil count below 500 million neutrophils per cubic liter of blood while a fever is declared at a body temperature of 38 degrees Celsius or greater. The details of the UK ALL 2011 protocol are very important in understanding how the state of FN occurred in the patient, because six of the eleven drugs used in the patient’s chemotherapy are myelosuppressive agents. Those drugs, which can all be seen in table 1, are daunorubicin, cyclophosphamide, cytarabine, mercaptopurine, methotrexate, and doxorubicin (4). These myelosuppressive agents may be cytotoxic to myeloid stem cells or their progenitors. Additionally, some chemical agents affect hematopoiesis directly (5). While the mechanism of action is not always known, statistical significance in practice and animal-model experiments make all of the above agents known myelosuppressors. Notable among these drugs are the anthracyclines daunorubicin and doxorubicin, both fermentation products of the bacteria Streptomyces peucetius var. caesius. Anthracyclines are known myelosuppressors, in fact, myelosuppression is the dose-limiting factor in anthracycline chemotherapy treatments. (6)
While it is valuable to have assurance that the diagnosis is not surprising given the patient’s circumstances, the cause of FN is not always very important relative to the treatment. The source of infection is not related to the standard treatment of FN unless the patient is diagnosed with a fungal infection. At presentation of FN, standard treatment requires a peripheral blood culture to be taken, blood to be taken for venous lactate levels, and routinely checking CRP and albumin. Urine should be sent for children below the age of five, as was done for the patient as well as a stool sample (7). A sputum microscopy and culture are also useful when sputum is present, as it was for this patient. Additionally, chest radiographs are sometimes useful when infection is suspected in the lungs, however they are not recommended without cause for suspicion as to the specified infection location and the patient did not receive a chest radiograph. After 48 hours, low risk patients can be considered for switching to oral antibiotics and outpatient therapy (7,8).
The patient was given Tazocin, which is a combination of piperacillin and tazobactam. The patient was also given gentamicin and septrin, which is a mixture of sulfamethoxazole and trimethoprim. This spattering of antibiotics, all targeting different types of bacteria, is standard for treating FN. Due to the severity and relatively high mortality rates of FN, it is better to cover all possibilities of organisms quickly. Even identifying one source of infection does not rule out the possibility of another infection, since a patient with neutropenia is severely immunocompromised. The patient’s treatment was standard to guidelines in that treatment of the fever was broad and intensive, as the major and immediate concern is to treat the fever.
REFLECTION:
This case gave me a great deal of knowledge and insight into the life of a patient with B-ALL. This 4-week pediatric rotation was an immense learning experience for me. Not only was I able to meet a lovely patient that was suffering from B-ALL, I also gained valuable knowledge and skills in how to obtain correct information through a collateral history. I spoke to and learned from the patient’s mother. Being able to obtain accurate information from the patient’s family was a skill I was able to develop during this rotation. I was also able to carry out pediatric examinations and elicit key signs and symptoms.
This rotation was not similar to clinical rotations I have had in the past. Finding a way to make the child comfortable such as playing pretend with a dinosaur, or showing interest in his tablet video games, was key before taking the relevant history. Building a rapport with children is a skill in itself. Developing a good bedside manner and being able to communicate to both parent and child is not always easy and I struggled to understand it when I was first exposed. As our mentors taught us, ignoring the child to receive the history from guardians will not be taken well by parents. As always, it is a balancing act.
When I first met this patient, he looked pale and weary to communicate to any doctors. It was clear that the child was tired of the relentless visits to the hospital for treatment and invasive procedures. Not only was the child tired of the hospital setting and doctors all around, but the patient’s parents were as well. The weekly blood tests and procedures were causing a decline in his emotional well-being. He was restless and tired of the same hospital scenery with the same video and board games in front of him. The mention of discharge relieved both mother and son. The first ten minutes of our encounter were spent having him show me a video game on his tablet. This relieved both the patient and his mother and made them feel more relaxed.
Another crucial learning point for me was how rigorous the treatment for leukemia can be. The patient had to come in for regular tests, transfusions, and lumbar punctures. This illness had taken over the family’s life. This can also cause social issues. The patient is now 4 and half years old and has been in and out of a hospital for a significant amount of his life. As normal healthy children his age are in pre-school, learning to play with children his own age, this patient is not. From a mental health perspective, this patient may be too young to understand the concept of mortality; but it is always important for us as physicians to ask that question. How much can they understand? Another important aspect is the parent’s mental health. They are socially isolated as well, with this illness taking over as much of their lives as well. It is never easy to break the news of cancer to a family. They will have many emotions, questions and concerns. Our job is to do the best we can to support and uplift them every step of the way.
Discussion and Reflection word count: 1513 words
REFERENCES:
- Dr. Rachel Hough. Acute lymphoblastic leukaemia (ALL) in children and young adults up to 16 years. Pages 39-41. Bloodwise.org.uk. September 2015. https://bloodwise.org.uk/sites/default/files/documents/chALL_patient_info_booklet.pdf
- PTC list of approved chemotherapy regimens 2015. London Cancer Alliance. Page 1. http://www.londoncanceralliance.nhs.uk/media/101869/pct-list-of-approved-chemotherapy-regimens-2015.pdf
- Rasmy A, Amal A, Fotih S and Selwi W. Febrile Neutropenia in Cancer Patient: Epidemiology, Microbiology, Pathophysiology and Management; August 2016; https://medcraveonline.com/JCPCR/JCPCR-05-00165
- Myelosuppressive Agents; Drugbank Website; https://www.drugbank.ca/categories/DBCAT002716
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "pediatric"
Pediatric nursing is the practice of nursing with children, youth, and their families across the health continuum, including health promotion, illness management, and health restoration. Pediatric nursing is not only centered on child care, but involves the well being of the family.
Related Articles
