
Essay Question: What do you think about the prospect of a $5 fee to see a GP?
The topic of a $5 patient co-payment for GP visits is an ongoing debate that is currently being argued from individuals to health care providers. Under this proposal, pensioners and concession card holders are exempted, and families are allowed 12 bulk billed visits before co-payment applies. So, why would the government slug patients with a $5 co-payment for GP visits? The Australian Centre for Health Research (ACHR, 2013) claims that by implementing this proposal, the government would save an approximate $750 million over 4 years and that the co-payment proposal would:
- Reduce avoidable demand for GP services
- Reduce incentives for GPs to over-service
- Remind people GPs are not free
- Reduce moral hazard risk by making people consider visiting a GP for minor ailments
- Remind people that maintaining good health is an individual’s responsibility
However in order to take a stance, it is important to first understand Health. Should Health be a right, or is it a privilege? If Health is a privilege, health insurance would only support emergencies and not day-to-day healthcare maintenance, which would be detrimental to those in financial hardship (J L. Marshall, 2011). Hence, Health should be a right, a right “based on need and not the ability to pay”, where everyone can have equal accessibility and treatment to health care, which is why the $5 co-payment should not proceed (Public Health Association Australia, 2011).
Expenditures and efficiency
So why does the government intend to cut expenses from the health sector through a co-payment? Are we spending too much? According to the Australian Institute of Health and Welfare – AIHW (2013), total health care expenditure in 2011-2012 amounted to $140.2 billion, which is 7.6% higher compared to the previous year (AIHW, 2013). Since GP visits are covered by Medicare, which is funded by the Government and through a levy, GP visits would be included in this $140.2 billion. However, it was reported that the total Medicare expenditure was $16.3 billion in 2010-2011, “total” meaning that it included GP visit along with various services covered by Medicare Benefits Schedule – MBS (Australian Government – Department of Human Resources, 2011). Thus, it is reasonable to consider that Medicare is only a small portion of the total expenditure.
According to The Organisation for Economic Co-operation and Development (OECD), Australia’s health expenditure stands at $3800 per person, which is 8.9% of the Gross Domestic Product – GDP. In comparison, USA’s health expenditure per capita was $8508 per person, or 17.7% of GDP. Does this perhaps mean that life expectancy in USA is better due to the extra cost to health care? This does not seem to be the case, but rather statistics demonstrates that the highly privatised health care system is inefficient as shown in Figure 1.

From Figure 1, by comparing USA to Australia or Canada, it shows that USA has a slightly lower life expectancy, but the health spending is almost double the figures of Australia and Canada’s. It should be noted that both Australia and Canada have universal health care systems in contrast to the privatised health care in USA.
Given that a privatised system is evidently less efficient but yet costs more for individuals, would it then be wise to implement the co-payment, a move seen by many as a means to slowly “dismantle” Medicare (C King, 2014)? According to Catherine King (2014), the government would reduce expenditure for healthcare by means testing Medicare, but Australians will have to carry the tab. Means testing access to primary healthcare will lead to greater privatisation, which will restrict access to GPs for most Australians, more so on older people, the vulnerable ones in our population and families with children (C King, 2014). King (2014) states that “GPs are the cheapest within health systems, experts at diagnosis and able to detect potential health issues in their infancy”. Thus, if GPs are restricted, people would end up in hospitals, the expensive side of the health care system, increasing the expenditure rather than saving.
Reduce avoidable demand for GP services
Besides the intention of cutting costs for health care, one of the reasons provided by the ACHR for the co-payment proposal was to reduce avoidable demand (over usage) of GP services. However, the solution to this issue would not be to introduce a $5 co-payment for GP visits, as there are concerns that the co-payment would “jeopardise equitable access to clinically appropriate healthcare” (J Swan, 2013). This can be explained with a few questions by considering the targeted audience and the effects of the solution:
|
Issue: Over usage of GP services
|
Solution: Introducing a co-payment
|
According to J Swan’s article “John Glover voices fears GP fee will make poor suffer” (2013), Professor Glover, who led Australia’s most detailed analysis on the relationship between a person’s wealth and their willingness to visit a doctor, states that there is “very strong” evidence that poorer people are already under using healthcare in proportion to their level of illness. Through his analysis, it is shown that only 5% of residents who lives among Sydney’s wealthiest neighbourhoods – Mosman, Woollahra and Hunters Hill, claimed they had delayed medical consultation due to financial issues. In contrast to less wealthy areas, Penrith had 13.5%; Nambour 23.4% and Ballarat had 17.9% residents claiming they would delay visiting doctors due to cost.
From these statistics, it is clear that the poor would be most affected. John Glover, director of the public health information development unit at the University of Adelaide describes that the $5 co-payment for doctor visits would “discourage the wrong group of people from visiting the doctor while doing nothing to dissuade those who are already over using GP services” (J Swan, 2013). The co-payment would cause those likely to get seriously ill to unreasonably avoid preventative care which is a step towards reducing what we have as a universal healthcare system – privatisiation (J Swan, 2013).
Disadvantage to certain group of people (delay seeking medical help)
Would the $5 co-payment disadvantage certain groups of people? The co-payment would have dangerous consequences for the poorest and sickest
This then comes down to the issue of cost and equity. Health Program director of Grattan Institute, Stephen Duckett states that “In the healthcare system there’s a trade-off between costs and equity, the government might save money in the short-term at the cost of equity, but Emergency departments would soon fill up with patients delaying to visit GPs” (J Swan, 2013).
Clogging up ED (caused by delay in seeking aid from primary health care)
Potentially preventable hospitalisations (PPH) have been defined as those hospitalisations which could have been avoided with access to quality primary care and preventative care. Rates of PPH for selected conditions, such as chronic conditions and vaccine preventable conditions are being used nationally and internationally as an indirect measure of problems with access to care and effective primary care.
In contrast it is well established that hospital admissions can be prevented by primary care. Australian data show that there are around 33 hospitalisations per 1000 people per year or 10% of hospitalisations could be prevented by effective primary care5. These primary care preventable hospital admissions are increasing in recent years. The ACHR report suggests that the introduction of a co-payment will reduce all GP attendances, both those regarded as necessary, and those that are perceived as unnecessary1. There are inadequate data to know how this will affect hospital admissions. However, the co-payment may increase rather than reduce overall government health expenditure.
I support the reasoning provided by ACHR for the introduction of co-payment to remind people that maintaining good health is an individual’s responsibility, which requires investments in comprehensive primary health care (Public Health Association Australia (2011). I also support the overall aim that health care expenditures must be properly managed, to ensure an accessible, equitable, safe, effective and efficient health service provision (Public Health Association Australia, 2011). However, introducing co-payments for GP visits is just one of many solutions available to reduce Health expenditures. Is it a good solution for the reasons provided by ACHR? In my opinion, I do not think it is a good solution. The co-payment would disadvantage the poor, ill and families with children greatly. It is an inefficient method not only to increase health care funding, but ineffective mechanism for reducing demand. The introduction of a co-payment for GP visits is a regressive move towards a privatised system. Given that a privatised system has been shown to be inefficient, “means testing and privatisation would only spell the end of Medicare and it’s not how the government should manage health expenditure” (C King, 2014). It is my belief that this proposal has been inadequately investigated and more research would reveal better options to constrain health expenditure while encouraging individual responsibility for health. If further investigation are to be carried out, I would strongly recommend the government look into the management of successful countries with universal health care system such as Canada; or they could make slight adjustments to the Medicare levy, which would help increase health funding as well.
References:
Jonathan Swan (2013, December 31). “John Glover voices fears GP fee will make poor suffer”. Retrieved 13 March 2014, from http://www.smh.com.au/federal-politics/political-news/john-glover-voices-fears-gp-fee-will-make-poor-suffer-20131231-304go.html#ixzz2p8w8aZ3vAs
Australian Centre for Health Research (2013, October 18). “A PROPOSAL FOR AFFORDABLE COST SHARING FOR GP SERVICES FUNDED BY MEDICARE” Retrieved March 18, 2014, from http://www.cormorant.net.au/images/18%20oct%202013%20achr%20gp%20copayment%20paper%20final.pdf
Sue Dunlevy (2013, December 29). “Health groups fear $5 GP will hit hospital emergency departments”. News Corp Australia Network. Retrieved 18 March 2014, from http://www.news.com.au/lifestyle/health/health-groups-fear-5-gp-fee-will-hit-hospital-emergency-departments/story-fneuz9ev-1226791543887
John L. Marshall (2011, February 3). “Is Healthcare a Right or a Privilege?”. Retrieved 20 March 2014, from http://www.medscape.com/viewarticle/736705
Public Health Association Australia (2011, September). “Policy-at-a-glance – Primary Health Care Policy”. Retrieved 20 March 2014, from http://www.phaa.net.au/policyStatementsInterim.php#p
Australian Institute of Health and Welfare (AIHW, 2013). “Health expenditure Australia 2011–12”. Health and welfare expenditure series no. 50. Cat. no. HWE 59. Canberra: AIHW.
Australian Government – Department of Human Resources (2011, July 8). “Medicare Australia Annual Report 2010-11”. Retrieved 25 March 2014, from http://www.humanservices.gov.au/spw/corporate/publications-and-resources/annual-report/resources/1011/medicare-australia-annual-report-2010-11-full-report.pdf
OECD (2013). “Health at a Glance 2013: OECD Indicators”. OECD Publishing. Retrieved 5 April 2014, from http://dx.doi.org/10.1787/health_glance-2013-en
Catherine King (2014, February 24). “GP co-payment would man the end of Medicare”. Retrieved 7 April 2014, from http://www.alp.org.au/gp_co_payment_would_mean_the_end_of_medicare
- What are the equity arguments against the proposal? Unfair to poor and frequently ill people
- What are the literatures from overseas on this topic?
Supporting evidence:
University of Adelaide expert on health inequality Professor John Glover
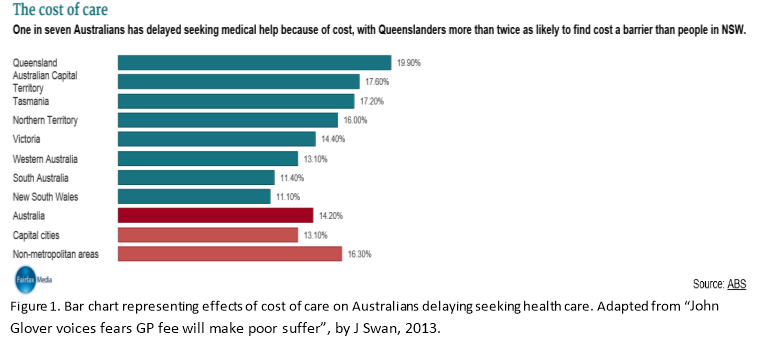
Report: The cost of care
One in seven Australians has delayed seeking medical help because of cost, with Queenslanders more than twice as likely to find cost a barrier than people in NSW.
Increased Ambulatory Care Copayments and Hospitalizations among the Elderly
Amal N. Trivedi (M.D., M.P.H)
- increasing the patient’s share of the cost for ambulatory care may not reduce (or may even increase) total health care spending and may result in worse health outcomes. Elderly patients may be particularly sensitive to cost sharing because they have lower incomes, are more likely to be in poor health, and have greater out-of-pocket spending on health care than nonelderly populations
- In conclusion, increasing copayments for ambulatory care reduced the use of outpatient care among elderly enrollees in managed-care plans, but this decline was offset by an increase in hospitalizations, particularly among enrollees with low socioeconomic status and those with chronic disease. Increasing copayments for ambulatory care among elderly patients may have adverse health consequences and may increase spending for health care.
http://www.nejm.org/doi/full/10.1056/nejmsa0904533#t=articleTop accessed date 13/3/2014
intro (250)
para 1 (650)
para 2 (650)
para 3 (650)
conclu (350)
(2550)
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "policy"
A healthcare policy is a set of rules and regulations that are put into effect to assist in the operation and the shape of health delivery. A healthcare policy covers a range of issues including public health, chronic illness and disability, long-term care, the financing of health care, preventive health care and mental health.
Related Articles
