
Environmental Assessment
The target population for this community needs assessment is those who have cardiovascular disease and qualify for cardiac rehabilitation. In order for a patient to receive the treatment of a cardiac rehabilitation program, one must have a qualifying diagnosis. This program is for patients who have systolic heart failure with an ejection fraction that is less than or equal to thirty-five percent, myocardial infarctions, status post percutaneous coronary intervention (stenting), heart valve replacement and/or repairs, status post coronary artery bypass surgery, or stable angina pectoris with a positive stress test (Phurrough, Salive, Baldwin, McClain, Schott, & Chin, 2006). Cardiac rehabilitation is a wellness program. A patient is connected to a 3-lead heart monitor that transmits the electrocardiogram to a computer that has a staff member monitoring while the patient is exercising. The patient will exercise between thirty-one to sixty minutes of exercise per session, for one to five days per week for thirty-six sessions. This program is referred by the patient’s cardiologist who signs off their individualized treatment plans every thirty days. While several people do qualify for cardiac rehabilitation and insurance coverage of the program, a number of people choose not to participate in the program.
The demographics of cardiac rehabilitation patients can greatly vary from low socioeconomic class to upper socioeconomic class. It also does not discriminate against any race or ethnicity, although certain ones are more common than others. Because cardiovascular disease affects several people across the globe, cardiac rehabilitation is the same way.
Social Assessment
Geographic boundaries of the community are nation-wide as it affects an array of people across the country of the United States of America. This particular needs assessment focused on the cardiac rehabilitation program that is located in Dallas, Texas at Texas Health Presbyterian Hospital of Dallas, where majority of the target community is from. The outlier cities include, Richardson, Desoto, Garland, Mesquite, and Forney, which are all cities surrounding Dallas.
Cardiac rehabilitations have been in existence since 1968 (Mampuya, 2012). Although exercise after the discovery of a cardiovascular disease diagnosis tried to begin in 1772, but set backs and a lack of studies proved to take a long toll to prove that exercise does in fact improve one’s cardiovascular disease (Mampuya, 2012). There are rehabilitation programs all across the United States of America and are also in other countries as well.
The number of cardiac rehabilitation programs in Dallas is unique compared to other cities in the state of Texas. While most cities have one option for a cardiac rehabilitation program, Dallas offers seven different locations. This can be due to the fact that there are several hospitals that are located in the city of Dallas, and the number of cities that feed into those hospitals.
Population size for cardiovascular disease can be a tough one to measure because there are several different types of diagnosis’s that go along with it. Although Centers for Disease Control and Prevention (CDC) states that there are an estimated 1.5 million heart attacks per year (Ritchey, Wall, Gillespie, George, Jamal, 2014). When doing research, it was shown that there is “one acute cardiovascular event in between 500 to 3900 adults each year” (Ryg 2015). However, it is predicted that by 2030, there will be forty and a half percent of the population will have cardiovascular disease (Heidenreich, Trogdon, Khavjou, Butler, Dracup, Ezekowitz, Finklestein, … Woo, 2011).
Key people and leaders of this community would be staff of the cardiac rehabilitation program, cardiologists, thoracic surgeons, those affected by cardiovascular disease, and hospitals. Each person has their own objective as to why this program is important to them and how they can improve quality of life. For example, cardiologist only want what is best for their patients and want them to succeed and get well. By having them do cardiac rehabilitation, a patient can have more responsibility in their own health, learn several health lifestyle tactics, and most importantly being monitored with their electrocardiogram rhythms, it is safer and known to catch an abnormality. Hospitals also benefit from this as well because they track the amount of times a patient gets readmitted and if they are readmitted for the same diagnosis. By using this program, the readmission rates, mortality, and morbidity rates have decreased.
Issues of most concern to the community of cardiac rehabilitation would be cardiovascular disease and the bettering of their health. When researching cardiovascular disease, there are several sub-diagnosis’s that can also occur along with it. For example, it is common for a patient with cardiovascular disease to have diabetes, high blood pressure, and high cholesterol levels. But with exercise, one can hopefully start to lower all of these levels.
A major resource that cardiac rehabilitation programs use would be the American Association of Cardiovascular and Pulmonary Rehab. And within that association, the state of Texas has its own branch with guidelines called the Texas Association of Cardiovascular and Pulmonary Rehab, where a conference is held every Socioeconomic Status
One of the risk factors for cardiovascular disease is stress management. When examining stress management, a big source of it would be the workforce. Many people experience stress from their place of work because of several different factors. It could either be the job itself is stressful due to the pressure or having to provide for oneself or family. According to Thayer, Yamamoto, & Brosschot (2010), the stress that work has on people affect their heart rate variability, this is especially prevalent in the older population because as time goes on there are changes that are made, whether technological or otherwise, that is hard for them to adapt. Retirement can also cause a major source of stress. Considering that those aged sixty-five years of age or older are either in their retirement phase or trying to get there soon, their income is priority.
Socioeconomic status
Another issue that arises with socioeconomic status and cardiovascular disease with the older population is affordability of treatment. Many people sixty-five years of age and older are on a fixed income from retirement from social security. They also usually have Medicare as their primary insurance. With healthcare being exceptionally expensive now-a-days, it is harder for people to afford the treatment that they so desperately need. This includes medications, screenings, and procedures to help their hearts be healthy and stay healthy. If healthcare becomes more affordable, more people would acquire the help they need to either prevent cardiovascular disease initially, prevent it from reoccurring, or decrease the mortality rate of the disease. According to Benjamin et al., (2017), in the year 2012 to 2013, cardiovascular disease and stroke made up a total of fourteen percent of the health expenditures cost. This is the largest expenditure cost of the year compared to other health diseases and issues. It is also predicted that the total expenditure costs in the year 2030 will be 918 billion dollars which is a 522 billion dollar difference from the total health expenditures in 2012 for cardiovascular disease (Benjamin et al., 2017).
Knowing those statistics, it shows how much people are spending on their health and not everyone is able to spend that amount of money. It is also discouraging to know that even with all the modern medicine, healthcare is still hard to come by unless you are of the upper class of the socioeconomic class. If the United States can come together to lower the costs of healthcare expenses, then more people would be able to obtain the treatment they need, and the mortality rate will in turn decrease over time. year for education purposes.
Gate Keeper Interviews
An individual that was interviewed for as a gatekeeper for this needs assessment was Vanessa Gonzalez, a physical therapist by trade but is the manager of the cardiac rehabilitation program at Texas Health Presbyterian Hospital of Dallas. She has been with this hospital for over ten years but, has been the manager of both the outpatient physical therapy and cardiac rehabilitation programs for the last four years. I chose to listen to listen to this particular person because she has a direct effect on the population of cardiac rehabilitation patients in the city of Dallas. The method used to interview her was a combination of an email sent to her with specific questions and a face to face interview as well to obtain more details of her answers.
The quality of life issues that she described for the cardiac rehabilitation community that she felt were important were psychosocial aspects of health, access to quality healthcare, and overall health of the patient. Psychosocial health is a major component in patients who are in cardiac rehabilitation. She went into detail how these patients and their families just went through an extreme life altering event and are now having to deal with the lifestyle changes and the outcomes from it. Most people do not understand or know how to deal with these emotions, so in cardiac rehabilitation, she stresses is a good outlet for both the patient and family members. Not only in the sense of exercise as medicine but also with expressing emotions and working out the lifestyle changes with the clinicians. Venessa also explained that access to quality healthcare is tremendously important to a person’s health care treatment. If one does not seek the quality of treatment they need for their cardiovascular disease it could be fatal for the patient. Venessa stated that cardiovascular disease and diabetes were the top two health issues that she feels affect this community the most. Several factors affect this, but one main one she discussed was the level of education. Education is a crucial component to any step in someone’s healthcare, but especially in cardiac rehabilitation. She expressed how far along this facility has come to making greater efforts for the education program. But she still sees room for improvement.
Another individual that was interviewed as a gatekeeper for cardiac rehabilitation was Susan Rodder, a dietitian for Texas Health Presbyterian Hospital of Dallas and a professor at UT Southwestern in Dallas. She has been working here for over ten years and sees cardiac rehabilitation patients once a week one on one to give them individualized care. Since she is only at this location once a week and is seeing patients, the best method to reach her is through her email. She was asked six different questions. When asked what type of health promotion programs she would like to see offered in this community, she answered emotional support programs for both patients and family members. The important health issue that the she believes the community is facing is the level of obesity which increase rate of chronic illnesses. Susan stated that making it easier to walk and ride bikes, reducing temptation of higher calorie foods are important issues that the community needs to address to create better lifestyle habits. Along with that she feels Dallas has made strides in creating better trails for people to exercise but, believes there should be more of a cap on the fast food and dessert options around town and replaced wit healthier eating choices. Susan stated that she participated in the American Heart Association community task force where she was able to provide more dietitians the perspective of what cardiac rehabilitation and cardiac patients in general go through. When asked the best way to communicate messages about a health issue in the community, she stated that events like the American Heart Association Heart walk, health fairs, and adding education areas at pharmacies are great ways to reach the public.
Epidemiological, Behavioral, & Environmental Assessment
The most pressing health issue for this community is heart disease, diabetes, and high blood pressure. Researching cardiovascular disease and comparing the State of Texas to the United states is depicted in Graph 1. It shows that Texas is one of the states that has the highest rate for death caused by Heart Disease (CDC, 2017).

Biologic Factors: Genetics
It is known that family history plays a major role in cardiovascular disease. According to American College of Sports Medicine (ACSM) (Pescatello, Arena, Riebe, & Thompson, 2014), that if a person’s biological father has had a heart attack before the age of fiftey-five then it will be a risk for a heart attack. The same goes for a person’s biological mother, if she has a heart attack before the age of sixty-five, then it will be considered a risk factor for that person that they will have cardiovascular disease as well. Cardiovascular disease has a large amount to do with cholesterol levels as well. According to the ACSM Guidelines (2014), if one’s cholesterol levels are a total great than 200 mg/dL or one has a high-density lipoprotein (HDL) level of 130 mg/dL, if one’s low-density lipoprotein (LDL) level is great than 130 mg/dL, then that is another risk factor that the person will have cardiovascular disease. While some people can control their cholesterol levels well with monitoring their diet and exercise, some people are predisposed to higher levels due to their genetics.
The national statistics from the World Health Organization (WHO) (World Health Organization, 2017), state that the total cardiovascular disease hospitalization rate per 1,000 Medicare beneficiaries aged sixty-five and older vary between races. For example, black American have an average 242.4 per 1,000, white Americans average 178.9 per 1,000, and Hispanics average 165.7 per 1,000 (WHO, 2017). This goes to show black Americans are more at risk from dying from the diagnosis of cardiovascular disease than compared to the other ethnicities.
When researching the comorbidities that can accompany cardiovascular, such as diabetes, it shows that in the state of Texas in Dallas county, of those aged 20 years of age or older, fifty six percent of them are diagnosed with diabetes (Centers for Disease Control, 2016). It also states that in Dallas county those aged 20 years of age and older are considered obese amounts to 55 percent of the population (Centers for Disease Control, 2016). And that 49 percent of the population is labeled as physical inactive because they do not receive more than 150 minutes of exercise per week (Centers for Disease Control, 2016). Knowing this information, one can see why cardiovascular disease is a major part of people’s lives and why it is so common.
PART 2
Precede Phase 3:
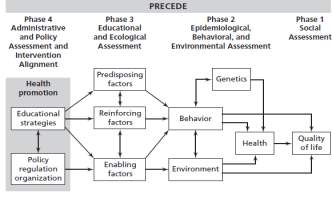
The PRECEDE-PROCEED model is widely used in the healthcare community when starting a new program. PRECEDE is an acronym for Predisposing, Reinforcing, and Enabling Constructs in Educational/Environmental Diagnosis and Evaluation (Community Tool Kit, 2018). There are four phases to the PRECEDE model. Phase 1 is identifying the definitive end goal, phase two identifying the issues that will conflict with that goal that are within the environment of the target community, phase three is identifying the predisposing factors that affect the behaviors and attitudes of the target population, and phase four is identifying the factors that can affect the outcome of the end goal (Community Tool Kit, 2018).
The predisposing issues for those with cardiovascular disease would be the mindset that it would “never happen to me” or that “I can eat whatever I want”. This way of thinking can cause people to not pay attention to the side effects of unhealthy habits.
Reinforcing of the behavior would be seeing others indulging in the bad behaviors that lead to cardiovascular disease such as bad eating habits, low physical activity, and low quality of life. This lifestyle can be passed down from family members, friends, or watching celebrities.
Enabling factors are the availability of fast food restaurants on every corner and several within that corner. The cost of health eating being expensive. With Americans wanting everything quick, easy, and accessible, the health aspect can often times get left behind. This is why fast food restaurants are in popular demand and why the obesity levels in America continue to rise and become more normalized over time.
Below is depicted a PRECEDE model. Phase one of PRECEDE model is about quality of life and the end goal of the intervention. For this particular community the end goal is to increase their quality of life by allowing them have more independence, possibly decrease some of their heart medications, and make them physically active. Phase two discusses the epidemiological assessment, which includes the health of cardiovascular disease, genetics attributable to the disease, behaviors that attribute to it, and the environment as well. For this community the health of the patients is those diagnosed with cardiovascular disease, the genetics are a possible predisposition because they are a major contributing factor. The behavior of not exercising and not eating well contribute, as well as the environment of having too many unhealthy options, too many services that do not require a person to get up and get moving. Phase four is about the predisposing factors, reinforcing factors that allow a patient to not change, and enabling factors. The predisposing factors of genetics is a major factor because one cannot change their genetics no matter how healthy they are. Reinforcing factors such as family or peers attributing the same unhealthy behaviors. Enabling factors are common because of the easy access to bad eating choices and bad physical inactivity choices. Below is depicted a PRECEDE model for cardiovascular disease.



Phase 3
Phase 2
Phase 1

Predisposing
“It won’t happen to me”
“I can eat whatever I want”
Genetics
High blood pressure
High cholesterol








Behavior
Bad eating
No physical activity
CVD
Chronic Heart Failure
Myocardial Infarction
Increase quality of life of CVD

Reinforcing
Peers who eat poorly
Family who does not exercise



Environment
Food Accessibility
Nearby parks



Enabling
Fast food availability
Expensive healthy food
Part 3
Pilot Study
The pilot study was taken place at Texas Health Presbyterian Hospital of Dallas in the cardiac rehabilitation program. It included the participation of twenty-four current cardiac rehabilitation patients. The method used for this study was handing out a survey to the patients asking them questions about their community, their healthcare providers, and their demographics. There were a total of seventeen questions that were asked and the survey that was given was adapted from the example source of survey given by the Health Studies Class. It was modified by adding three questions about their health care providers and adding on the age range to 85. When asking questions about their demographics, majority of the patients have a household income of over $50,000 a year and use the health insurance Medicare to pay for their medical expenses. The age range was from 40 years old to over 85 years old. Patients also identify as African American (1), Hispanic Latino (3), White/Caucasian (18), and other (1) as shown in Table 10. In Table 1, it shows that important health community factors are a good place to raise children (11), low crime/safe neighborhoods (15), and being in an area where there are good schools (10). These can be all be related to socioeconomic classes because normally the higher the class, the safer the neighborhoods. It also has to do with accessibility to health care. If one is able to afford to live in the “nicer” neighborhoods, then they most likely will be able to afford better quality and easier access to healthcare.
Table 1. “In the following list, what do you think are the three most important factors for a “Healthy Community”?”
| Category | Frequency | Total |
| Good Place to raise children | 11 | |
| Low crime/safe neighborhoods | 15 | |
| Good schools | 10 | |
| Access to health care | 6 | |
| Parks and recreation | 3 | |
| Clean environment | 6 | |
| Affordable housing | 2 | |
| Excellent race relations | 1 | |
| Good Jobs and healthy economy | 3 | |
| Strong family life | 5 | |
| Healthy behaviors and lifestyles | 5 | |
| Low infant deaths | 1 | |
| Religious or spiritual values | 4 |
*n=24
Table 2. “In the following list, what do you think are the 3 most important ‘health problems’ in our community?”
| Category | Frequency | Total |
| Aging problems | 9 | |
| Cancers | 8 | |
| Child abuse | 2 | |
| Diabetes | 12 | |
| Domestic violence | 4 | |
| Firearm-related injuries | 2 | |
| Heart disease and stroke | 16 | |
| High blood pressure | 11 | |
| Homicide | 1 | |
| Infectious diseases | 1 | |
| Mental health problems | 6 |
*n=24
Table 3. “In the following list, what do you think are the 3 most important ‘risky behaviors’ in our community?”
| Category | Frequency | Total |
|
Alcohol abuse
Being overweight |
8
14 |
|
| Dropping out of school | 4 | |
| Drug abuse | 11 | |
| Lack of exercise | 14 | |
| Poor eating habits | 11 | |
| Not getting “shots” to prevent disease | 5 | |
| Racism | 2 | |
| Tobacco use | 2 | |
| Other__mental health | 1 |
*n=24
Table 3. “ how would you rate our community as a ‘Healthy Community’?”
| Rating | Frequency | Total |
| Very Unhealthy | 1 | |
| Unhealthy | 1 | |
| Somewhat Healthy | 10 | |
| Healthy | 9 | |
| Extremely Healthy | 3 |
*n=24
Table 4. “How would you rate your own personal health?”
| Rating | Frequency | Total |
| Very Unhealthy | 1 | |
| Unhealthy | 0 | |
| Somewhat Healthy | 9 | |
| Healthy | 11 | |
| Extremely Healthy | 3 |
*n=24
Table 5. “How would you rate your overall understanding of your diagnosis?”
| Rating | Frequency | Total |
| Poor | 0 | |
| Fair | 3 | |
| Good | 8 | |
| Excellent | 13 |
*n=24
Table 6. “How would you rate your cardiologist responsiveness to calls?”
| Rating | Frequency | Total |
| Poor | 0 | |
| Fair | 1 | |
| Good | 6 | |
| Excellent | 17 |
*n=24
Table 7. “How would you rate your overall education that you receive from your healthcare provider?”
| Rating | Frequency | Total |
| Poor | 0 | |
| Fair | 1 | |
| Good | 9 | |
| Excellent | 14 |
*n=24
| Female | Male |
| 4 | 19 |
| Ethnic Group | Total |
| African American/Black | 1 |
| Asian/Pacific Islander | 0 |
| Hispanic/Latino | 3 |
| Native American | 0 |
| White/Caucasian | 18 |
| Other | 1 |
Table 8. Table 9. Table 10.
| Age | Total |
| 40-54 | 1 |
| 55-64 | 6 |
| 65-74 | 9 |
| 75-84 | 4 |
| 85 and over | 3 |
*n=23 n=23 *n=23
Discussion
A total number of 24 patients participated in this study (n=24), however one patient did not complete the demographic section of the survey. After reviewing the surveys, one would see that a majority of current cardiac rehabilitation are very satisfied with their healthcare providers on the education that they receive. Delving further into the surveys, I was able to ask additional follow up questions to some of the cardiac rehabilitation patients on how they felt their education was excellent. Majority of the patients stated that the cardiac rehabilitation staff as the healthcare provider gave excellent education and builds on the education from their cardiologists. And when asked if they felt if they would have gained this knowledge that they receive in cardiac rehabilitation, would they think they would have eventually known it, fifteen out of twenty patients stated no. This goes to show the importance of cardiac rehabilitation and how it not only affects their heart health, but affects their overall health and education.
Public Health Education Program
Public health education can affect the predisposing, reinforcing, and enabling factors by creating more attainable factors. One of the factors would be limiting the availability of unhealthy fast food chains and making fresh foods more affordable. This way people would be more inclined to buy fresh foods and less likely to buy greasy foods that will ultimately clog their arteries and cause cardiovascular disease.
Another health behavior model that would work well for this population would be the Transtheoretical Model. Using this model, a patient can be at any stage of change for their health behavior.
Good resources to help the community health educators for cardiac rehabilitation would be American Heart Association because they give easy to understand articles on several different topics that relate to cardiovascular disease. Another good resource would the AACVPR website. It helps people with their education that one would give to their patients or patients can use for themselves about cardiovascular disease and how to better themselves. Education is a major factor in cardiovascular disease and cardiac rehabilitation. One must never stop learning and researching the best ways to take care of themselves.
References
- #1 https://www.bmj.com/content/351/bmj.h5000.short :cardiac rehab stats
- Dalal, H. M., Doherty, P., & Taylor, R. S. (2015, September 29). Cardiac rehabilitation. Retrieved from https://www.bmj.com/content/351/bmj.h5000.short
- Benjamin, E., Blaha, M., Chiuve, S., Cushman, M., Das, S., Deo, R., … Munter, P. (2017). Heart disease and stroke statistics-2017 ppdate. PMC, 135(10), e146-e603. doi: 10.1161/CIR.0000000000000485
- #2 http://www.onlinejacc.org/content/accj/67/1/1.full.pdf : effective mortality of CR
- Community Tool Kit. (2018). Section 2. PRECEDE/PROCEED. Retrieved from https://ctb.ku.edu/en/table-contents/overview/other-models-promoting-community-health-and-development/preceder-proceder/main
- Pescatello, L. S., Arena, R., Riebe, D., & Thompson, P. D. (2014). ACSMs guidelines for exercise testing and prescription. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health.
- Ritchey, M. R., Wall, H. K., Gillespie, C., George, M. G., Jamal, A., (2014) Million Hearts: Prevalence of Leading Cardiovascular Disease Risk Factors — United States, 2005–2012. Centers for Disease Control and Prevention, 63(21);462-467. Retrieved from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6321a3.htm
- Ryg, J. W., (2015). American College of Sports Medicine (ACSM) Risk Factor Screening. Retrieved from: https://static1.squarespace.com/static/555658d8e4b07b37133355d4/t/55c8e9b8e4b03a2e8b316d01/1439230392475/Mend+ACSM+Cardiac+Screening+Article.pdf
- Heidenreich, P., Trogdon, J.Khavjou, O., Butler, J., Dracup, K., Ezekowitz, M., Finklestein,E., … Woo, J., (2011). Forecasting the future of cardiovascular disease in the United States, 933-944. DOI: 10.1161/CIR.0b013e31820a55f5
- Mampuya, W. M. (2012). Cardiac rehabilitation past, present and future: An overview. Cardiovascular Diagnosis and Therapy,2(1), 38-49. doi:10.3978/j.issn.2223-3652.2012.01.02
- Centers for Disease Control. (2016). Interactive Atlas of Heart Disease and Stroke. Retrieved from https://nccd.cdc.gov/DHDSPAtlas/Reports.aspx
- Phurrough, S., Salive, M., Baldwin, J., McClain, S., Schott, L., & Chin, J. (2006). Retrieved from https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=164&NcaName=Cardiac Rehabilitation Programs&DocID=CAG-00089R
- World Health Organization. (2017, May). Cardiovascular diseases (CVDs). Retrieved July 20, 2019, from https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
- Centers for Disease Control. (2017). Total Cardiovascular Disease and Death Rates [Map]. In Centers for Disease Control.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "cardiovascular disease"
Cardiovascular disease is a heart condition which involved the narrowing or blocked blood vessels that can lead to myocardial infarction, angina, or stroke. Other examples of cardiovascular diseases include atherosclerosis, coronary artery disease, peripheral artery disease, carotid artery disease, and arrythmias.
Related Articles
