
Introduction
A suture is any strand of material used to ligate blood vessels or approximate tissues. It consists of a thread material which is attached to a needle. The use of suturing has been documented as far back as 2000 B.C. by Egyptians. Today many see suturing as an art form in surgery. Dentists and surgeons alike should have a thorough understanding of the design of the equipment and materials they are using.
In dentistry, sutures are routinely used to achieve haemostasis, approximate tissues after extraction, implant surgeries, periodontal surgeries and biopsy procedures. Intra-orally most wounds heal by secondary intention which can delay the healing process and this can manifest clinically as symptomatic issues for patients. Suturing makes it possible to strive towards healing by primary intention. Suturing can also act as an adjunct to treatment, for example in periodontal crown lengthening surgery the primary aim is to remove excess tissue via incisions but the type of suturing can help reposition the tissues more apically.
This article aims to inform the reader of types of suture needles, suture materials and techniques which will provide an insight into material selection and overall better treatment outcomes based on a more educated approach.
|
Primary aims of suturing |
|
Approximate wound edges to maximise healing by primary intention |
|
To cover bone as much as possible to prevent bone necrosis |
|
Hold the flap in the desired position |
|
To aid in soft tissue haemostasis |
Table 1, Aims of suturing
The Anatomy of a Needle:
The Point
The point extends from the tip of the needle to the maximum cross-section of the needle body.
The Body
This is the portion of the needle that is held by the needle holder while suturing. The body diameter should match that of the suture material as closely as possible to bleeding and leakage. The shape of the body can vary greatly ranging from straight to fish-hook-shaped. Curved needles require less space for manoeuvring compared to a straight needle. Most commonly in dentistry, the curvature of the body is designed around a circle, typically these are 3/8 circle, 1/2 circle and 5/8 circle.
The Eye
There are three categories that the eye of a needle can fall into the closed eye, French or swaged (eyeless). The majority of needles used in surgery are swaged. With this configuration the needle and suture form one continuous unit which minimizes tissue trauma.
- Point
- Body
- Eye
3

2
1
Figure 1, Diagram of a suture needle
Needle Types
Conventional Cutting
This needle type has three cutting edges, the third being on the inside of the curvature of the needle. This type of needle may be prone to cutting out of tissue because the insidecutting edge cuts towards the edges of the incision.
Reverse Cutting
These needles were created for tough, difficult-to-penetrate tissue such as skin and oral mucosa. This needle is as sharp as the conventional cutting needle but its design is slightly different. The third edge is located on the outerconvex curvature of the needle. This offers several advantages such as:
- Reverse cutting needles have more strength than conventional cutting needles
- The danger of tissue tearing is greatly reduced
- The hole left by the needle leaves a wide wall of tissue for the suture to rest against while the suture is tied.
Taper-Point
Taper-point needles pierce and spread tissue without cutting it. The needle point tapers to a sharp point. The needle body flattens to an oval or rectangular shape. They are preferred when the smallest possible hole in the tissue and when minimum tissue cutting is desired.
Taper-Cutting
This needle combines the features of both the reverse cutting edge tip and taper point needles. The cutting edge extends slightly from the point and then blend into a round body. All three cutting edges are typically sharp to provide a uniform cutting action. The point (aka trocar) readily penetrates tough tissues.
- The point diameter should not exceed that of the suture
- The tapered body provides smooth passage through tissue.

Figure 2, Types of needles
|
Optimal suture qualities include: |
|
1. High uniform tensile strength, permitting the use of finer sizes. |
|
2. High tensile strength retention in vivo, holding the wound securely throughout the critical healing period, followed by rapid absorption. |
|
3. Consistent uniform diameter. |
|
4. Sterile. |
|
5. Pliable for ease of handling and knot security. |
|
6. Freedom from irritating substances or impurities for optimum tissue acceptance. |
|
7. Predictable performance. |
Table 2, Suture material Qualities

Figure 3, suture classification

Figure 4, Monofilament suture Figure 5, multifilament suture
|
Suture Type |
Absorbable |
Non-absorbable |
Natural |
Synthetic |
Monofilament |
Multifilament |
|
Vicryl |
X |
|
|
X |
|
X |
|
Silk |
|
X |
X |
|
|
X |
|
Chromic |
X |
|
X |
|
X |
|
|
Monocryl |
X |
|
|
X |
X |
|
|
Nylon |
|
X |
|
X |
X |
|
|
Prolene |
|
X |
|
X |
X |
|
Table 3, Suture types
Suture Materials
|
Suture Name |
Material |
Degradation |
Absorption Time
|
Tensile Strength |
Retention of Tensile Strength |
Tissue Response |
Uses |
|
Vicryl |
Polyglactin 910 |
Hydrolysis |
Complete between 56-70 days. |
Good |
Approximately 75% remains at two weeks. Approximately 50% remains at three weeks, 25% at four weeks.
|
Minimal acute inflammatory reaction
|
Intraoral closure of muco-periosteal flaps, post-biopsy closure and socket closure |
|
Vicryl Rapide |
Polyglactin 910 |
Hydrolysis |
Complete by 42 days |
Good |
50% remains at 5 days. All tensile strength is lost at approximately 14 days. |
Minimal to moderate acute inflammatory reaction
|
Same uses as Vicryl, not used when tissue requires a longer holding period for more stable healing Treated with gamma rays which increases the speed of absorption |
|
Silk |
Silk |
Non-absorbable |
Gradual encapsulation by fibrous connective tissue.
|
Excellent |
Progressive degradation of fibre may result in gradual loss of tensile strength over time. |
Acute inflammatory reaction
|
More durable intraoral sutures and due to cost of more commonly used sutures |
|
Chromic Catgut |
Chromic Catgut |
Phagocytosis and enzyme degradation |
Absorbed by proteolytic enzymatic digestive process. |
Poor-fair |
10-14 days |
Moderate reaction |
Surgical gut may be used in the presence of infection, although it may be absorbed more rapidly under this condition. |
|
Monocryl |
Poliglecaprone 25 |
Hydrolysis |
91-119 days |
Excellent |
Approximately, 50-60% remain (violet: 60-70%) s at 1 week. Approximately 20-30% (violet: 30-40%) remains at 2 weeks. Lost within 3 weeks (violet: 4 weeks).
|
Minimal acute inflammatory reaction
|
Microvascular closure in oral and maxillofacial surgery
|
|
Nylon |
Nylon |
Non-absorbable |
Gradual encapsulation By fibrous connective tissue. |
Excellent |
Progressive hydrolysis may result in gradual loss of tensile strength over time.
|
Minimal acute inflammatory reaction |
Extra-oral wound closure |
|
Prolene |
Polypropylene |
Non-absorbable |
- |
Excellent |
No subject to degradation or weakening by the action of tissue enzymes. |
Minimal acute inflammatory reaction
|
Intended for use as durable and long-lasting, mostly for extra-oral suturing |
|
Ethibond |
Polyethene terephthalate |
Non-absorbable |
Gradual encapsulation by fibrous connective tissue |
Excellent |
No significant change is known to occur |
Minimal acute inflammatory reaction |
|
Table 4, Suture materials and properties
Instruments
Needle Holder
Needle holders are used to position and pass the suture through tissues during suturing. They can come in many different designs with most needle holders having a ratchet to lock the suture needle in place. The needle holder is held with a palm grip to allow extension of thumb and fingers into the ring of needle holder to allow greater mobility of the suture needle.
Tissue forceps
Most often toothed tissue forceps are used to gently position tissues to allow perpendicular passage of the suture needle to ensure a rectangular flat knot can be made. The forceps can also be used to grasp the needle when repositioning it in needle holder to minimise the risk of percutaneous injury.

Figure 6, Instruments used in suturing
Suturing techniques
Simple Interrupted
This is the simplest and most common type of suture used in dentistry. Each simple interrupted suture is independent and multiple simple interrupted sutures can be placed in the same wound to gain better wound closure. It consists of a single thread passed through two separate ends of tissue tied by a knot. Advantages of these sutures are that can be used in areas where the tissues are under stress and when used in series the failure of one stitch does not necessarily mean the others will fail. It is most commonly used to prevent haemostasis post-extraction, close biopsy wound sites and close oro-mucosal flaps.

Figure 7, Simple interrupted sutures
Vertical Mattress
This type of suture is used to reduce the amount of dead space and provides an increased strength across the wound. It consists of two separate entries of the suture needle. Initially, a bite is taken 5-6mm from the wound on both ends of the wound then a second bite is taken 1-3mm from the wound edge on both sides and then tied on the initial entry end.







Figure 8, Vertical Mattress suture
Horizontal Mattress
This type of suture is useful in reducing tension across large wounds. It consists of insertion 5-6mm from the wound edge on one side and exiting at the same distance on the opposing side, then the needle is reintroduced 3-5mm from the wound edge on the second side and the suture exits from 3-5mm from wound edge on the first side and is tied with a knot.


Figure 9, Horizontal mattress suture
Simple Continuous
This type of suture is faster and relies on fewer knots which makes the suture inherently weaker. This suture has the ability to evenly spread the tension where the tissues are approximated. It consists of passing the needle through both tissues ends separately then rather than tying a knot like a simple interrupted the needle is reintroduced into the tissue at a more lateral position to the previous entry. The suture is then tied by using the primary insertion and the terminal exit portion of the thread. This type of suture is simple and fast and it distributes the lesion evenly across the incision line. However, a single point of failure in this suture may lead to total loosening and failure of the entire suture.
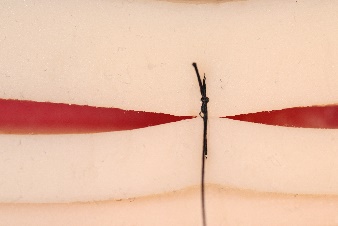
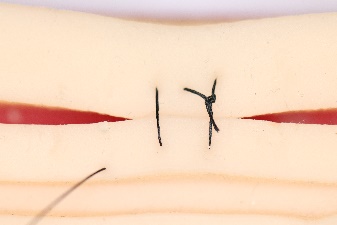


Figure 10, Continuous suture
Safety tips while suturing
For all its advantages suturing carries its own risk of percutaneous injuries. There are certain safety measures that can be taken to minimise the risk of such injuries. The primary technique is to minimise the amount of contact the surgeon's hands have with the needle, this can be minimised by using the toothed tissue forceps when repositioning the needle. Careful repositioning of the needle extra-orally can also minimise the risk of damage to the intra-oral tissues.
When cutting sutures using the scissors, the hand positioning should be similar to when holding a needle holder. The index finger should rest on the body of the scissors and the suture threads should be held taught using the needle holder and a point of contact along the thread should be established and a finger from weak hand be used to stabilise the scissors before cutting the thread.
After suturing is completed all sharps should be disposed of immediately. Sharps can be disposed of into a separate sharps bin or temporarily placed in a sharps bowl. The operator should dispose of their own sharps after they have completed the procedure. This will minimise percutaneous injuries for both the operator and assistants.
Emerging trends in suturing
Antimicrobial agent coated sutures
Triclosan-coated absorbable suture materials with antimicrobial properties are used to prevent postoperative infections. Triclosan is an antimicrobial agent that is commercially used in several products such as toothpaste. Triclosan-coated sutures effectively reduced bacterial growth while having no effect on bacterial adherence compared to standard sutures. This type of suture is commercially available (Vicryl Plus, Ethicon).
There has been other antimicrobial agents which when used to coat sutures have proved to be effective (e.g. chlorhexidine).
Drug-eluting sutures
The sustained release of drugs at a specific site can allow therapeutically relevant concentration locally for prolonged duration without exceeding toxic limit in the systemic circulation. When fabricating these types of sutures there is a fine balance between maintaining the desired mechanical characteristics of the suture and being able to obtain the required concentration and potency of the drug.
Fibrin Sealants
Fibrin sealant can be prepared from the patient’s own blood (autologous) or from donated blood. There are two components in a fibrin sealant, thrombin and fibrinogen when mixed form a fibrin clot. The aim of fibrin sealants is to approximate and retain wound edges, provide haemostasis and reinforce tissues through adherence. They can function as a haemostat, sealant or adhesive and they can enhance the overall clinical outcome of surgical treatments.
Barbed Sutures
Barbed sutures are currently being used in obstetric, orthopaedic and plastic surgery. These types of sutures allow for tissues to be approximated without tying knots. This is due to the configuration of barbs used, this being either bidirectional or unidirectional. Bidirectional barbed sutures have barbs in both directions, allowing one end of the suture to anchor the other without having to tie a knot. Unidirectional barbed sutures have barbs in a single direction secured by a looped end.

Barb’s present along suture, mechanically prevents back movement via design
Figure 10,Barbed Suture design
- Dennis, C. et al. (2016) ‘Suture materials — Current and emerging trends’, J Biomed Mater Res Part A, 104A, pp. 1544–1559. doi: 10.1002/jbm.a.35683.
- Domnick, E. D. (2014) ‘Suture Material and Needle Options in Oral and Periodontal Surgery’, J Vet Dent, 31(3).
- James R.Hupp, DMD, MD, J. (2015) ‘Journal Of Oral and Maxillofacial Surgery: Guide to Suturing’, Journal of Oral and Maxillofacial Surgery, 73(August).
- KG, S.-W. (ed.) Pocket guide: Suture Material Techniques & Knots. 6th Revise. Naila, Germany.
- Koshak, H. H. (2017) ‘Dental Suturing Materials and Techniques’, Glob J Otolaryngol, 12(2), pp. 1–11. doi: 10.19080/GJO.2017.12.555833.
- Modi, M. (2009) ‘Critical Evaluation of Suture Materials and Suturing Techniques in Implant Dentistry’, International Journal of Clinical Implant Dentisttry, 1(May-August), pp. 31–40.
- Sharif, M. O. and Coulthard, P. (2011) ‘Suturing : An Update for the General Dental Practitioner’, Dental Update, 38, pp. 329–334.
- Silverstein, L. H., Kurtzman, G. M. and Shatz, P. C. (2009) ‘SUTURING FOR OPTIMAL SOFT -TISSUE MANAGEMENT’, Journal of oral implantology, XXXV.
- patent:8795332,Barbed sutures,Leung, Jeffrey C. ,Ruff, Gregory L.,Megaro,MatthewA.,2014,August,http://www.freepatentsonline.com/8795332.html
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "dental"
Dentistry, also known as dental medicine and oral medicine, is a branch of medicine that consists of the study, diagnosis, prevention, and treatment of diseases, disorders, and conditions of the oral cavity.
Related Articles
