
How Culture Around The World Affects The Spread of STI’s and STD’s
ABSTRACT
STD/STI rates are not synonymous in every part of the world. There is a plethora of varying reasons as to why these differences exist, all of which fall under our umbrella term, culture. Culture in its most basic understanding engulfs all aspects of what we consider societal and what we understand about our internal and external environments. In this paper I will discuss sex, our one method of procreation, has definitively rooted itself in everyone’s culture, as it is as old as multicellular life itself. Because of the complexity and rapidity that culture transforms itself, our viewpoint on sex tends to do the same thing, mixing and meshing contrasting cultures that negatively impact one another in many instances. Religion vs non-religious, young vs old, and different regions and ethnicities, all bring varying sexual practices from their culture and thought processes that make or break sexual health in a community.
INTRODUCTION
Culture is the variety in our existence; culture is what has shaped society and the roles we fulfill within it since the inception of intelligent communication. Culture has proven to be ambivalent with its relationship to our well-being, as it has shaped the views and ideologies of many in positive and negative ways. Culture has facilitated the advancement of humanity, but with those improvements comes baggage from members of society who still hold on to what we know now to be detrimental practices, traditions, and thought processes. When it comes to the sector of sex in particular, some cultures are often reluctant and/or ignorant to the precautionary and preventive measures when it comes to sex. Society has proven throughout time to be imbalanced on its approach to sex culture, education, and stigma. Greek culture was one of the first recorded cultures that demonstrated influence on sex culture today, implementing and perpetuating a litany of, what for a long time was taboo, liberated sexual practices such as prostitution, pederasty, nymphomania, and others.
Between 400 AD and 1000 AD we witnessed Christian morality gain a grip on Western thought “so paralyzing that it is only now beginning to relax”, according to Reay Tannahill’s book Sex in History.1 Many of its rules and stipulations regarding sex withstood the test of time for over 1,500 years, with threats of hellfire for eternity proving one of the most successful deterrents ever established. Lust and sex became associated with the original sin of Adam and Eve and the celibate life was promoted for those with the godliest minds. An indication of how poorly early Christians viewed sex is the fact that they declared Jesus to have been conceived without carnal contact. Incest, masturbation, oral sex, anal sex and homosexuality were all deemed sinful and punishable by the Christian church with increasing severity. Sex within marriage was tolerated for reproductive purposes only and contraception banned because of its associations with pleasure. We know little of how these rules affected the lives of ordinary people, but the threat of damnation almost certainly transformed sex into an activity loaded with fear and danger, which for centuries has kept knowledge about sex in the shadows for those who need it the most. This ultimately led to the ignorance and tunnel vision view many people have on sex presently.
The sex revolution in the 1960’s appeared as a time for social change which lead to the change in sexual tendency, behavior and perception. Women’s burgeoning sexual freedom coupled with the rise of venereal diseases during the late 1960s, cultivated the ideology that women were the primary contributor of most sexually transmitted diseases and infections.2 However we now know that women are not the primary contributors to the spread and conception of many modern sexually transmitted diseases and infections but rather, the STD’s existed long before the late 1960’s and had not yet been identified. Certain practices and religions do more harm than good nowadays, especially when it comes to some of the disparities between certain areas that lack opportunity and access to healthcare. This then leads to the discussion of socio-economic status (SES) which can determine whether one is more susceptible to STD’s and STI’s or not. Also, back then people were perhaps more conservative, sex was not something that was free nor frequent as is today which can be a reason in upticks and up rises of today.
There has been a stigma lingering around when it comes to reporting or going to check if one has a STD or a STI amongst adolescence. Many often fear being judged or frowned upon. The access to sexual education amongst adolescents is sometimes limited, especially by region even within the United States. In the Southern States where they have adopted more conservative political viewpoints and promote abstinence-only sex education, you can see how these methods lead to an outcome where in a society where sex has not been liberated nor spoken of openly. Taught in a lackluster manner to children and teenagers in other regions, and is scattered in abundance all over the internet, the southern region has higher STD and teen pregnancy rates than anywhere else in the country.
The objectification of women has unfortunately allowed jobs like prostitution to become profitable options for low income women. Women and sometimes men are subjected to health standards and practices that promote the spread of STD’s and STI’s. Lower SES tends to have riskier environments. To make matters worse, these people are controlled, manipulated, and chances are they are all under scrutiny of friends, family and the law, reducing the chances sex workers and exploiters get checked for disease and infections. Women in particular have the tendencies to not show symptoms when they are infected.3 This is when STI’s spread, because by the time the symptoms show, the damage is already done. Because of the modern stigma concerning sexual health, more often than not, women are afraid or embarrassed to go to a physician and regularly get checked out because it may show that they are sexually promiscuous, which has been frowned upon by women and men for women exclusively in society.
Regulation of prostitution has also been a question that has been circulating. Some believe that if prostitution was to be regulated globally, the spread of STDs would increase because people would be under the presumption of being in a safe bubble and thinking that he/she environment is safer than it already is or because one is in a safe environment, he/she’s sexual activities becomes less risky. Illegalization may lead to more illegal and unsafe practices as well by people who may be willing to break the law to instill prostitution, brothels or sex work in general. This may be left in the hands of someone untrustworthy and therefore this may lead to fear of getting tested due to fear of law enforcement.
Religions, such as Christianity, is one of the dominant religions practiced around the world are known to implement celibacy and/or abstinence from sexual intercourse. This has not only shaped the way society thinks but also what is being taught in our schools here in the U.S. and globally.
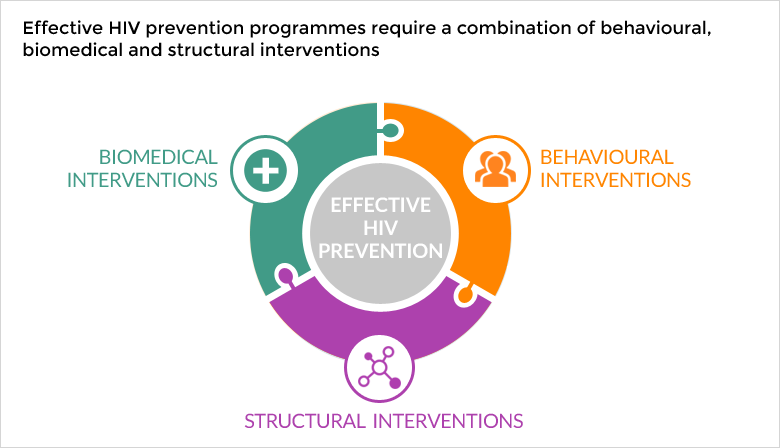 There have been implementations provided too communities to reduce the risk of contracting STDs and STI’s. As seen in Figure 1, an HIV prevention model has been put into place which tackles biomedical, behavioral, and structural interventions; each of these dealing with not only the individual, but the medications they consume and their environment as well.
There have been implementations provided too communities to reduce the risk of contracting STDs and STI’s. As seen in Figure 1, an HIV prevention model has been put into place which tackles biomedical, behavioral, and structural interventions; each of these dealing with not only the individual, but the medications they consume and their environment as well.
Figure 1: HIV Prevention Model used for interventions
METHODS
Upon doing this research, there is a plethora of sources that stood out when it came to giving statistical data and background on my topic of cultural effects on the spread of STDs and STIs. Articles under the National Center for Biotechnology and Information (NCBI) such as “Comparing the awareness of and beliefs in sexually transmitted infections among university students in Madagascar and the United States of America” and “Adolescents’ views of and preferences for sexual and reproductive health services in Burkina Faso, Ghana, Malawi and Uganda” focused on Ignorance to STI’s and HIV and AIDS as well as to why adolescents fear treatment and are also unaware of source to obtain treatment and contraceptives. The Center for Disease Control website discussed why STDs are not reported in some cases and why certain groups such as sex workers may be more prone to catch these illnesses. Government websites such as the World Health Organization and the U.S Department of Health and Human Services provided evidence for my research. A review done by James Pellerin and Michael B. Edmund spoke on rituals performed on the body to fulfill a religious obligation.
RESULTS
Young adults have reportedly been said to have a higher risk of contracting sexually transmitted infections than any other age group4. Because it has been thought that this may be due to social and cultural settings, a cross cultural study was done to study the relationship between culture in a place of study and STI awareness, beliefs in STI’s and self-reported STI prevalence in the study population 4. In this study, it was found that the students from Madagascar did not have a lower awareness of STIs than American students, however, there was disbeliefs in HIV/AIDs. The Students from Madagascar were also more likely to report having STI’s except for HIV and AIDS 4 . When looking at cure and awareness of sit 70% of Malagasy students listed that they had one STI and 74% of students in the United States listed the same . A higher percentage of Malagasy students reported disbelief in the existence of HIV/Aids than American students (15.4% and 4.0% of students in Madagascar and the United States, respectively)4. Once adjusting gender, place of study became an effect of this. There was also a reported difference in beliefs when it came to Syphilis and Gonorrhea. Although, not that much of a margin, students in the U.S has a disbelief in syphilis by 6-9% and for Malagasy students by 3.4%. As for Gonorrhea Malagasy students had a disbelief for this STI by 3.1% as compared to students in the U.S by 1.1%.4. When it came to the reason for disbelief, it was interesting to find that for the STIs that Malagasy students believed in 32.1% and 37.4% respectively accounted for Gonorrhea and Syphilis being real because they had seen , in contrast to American students believing in both infections by less than 10% (2.0% and 1.2% for syphilis and gonorrhea, respectively)4. It was also because the Malagasy students reported having these infections by as well. When it came to learning about Gonorrhea, Syphilis, and HIV/AIDs USA students reported learning about it more than Malagasy students. However, a large percentage of both USA and Malagasy students game no response as to why they held disbeliefs towards these three infections. But it was more prevalent amongst American students.
Throughout most parts of the world , prostitution is illegal (e.g. Belgium, South Africa, Canada and most of America).5 The only state in the U.s that has some form of legal prostitution is Nevada. It is said that sex workers in Nevada have to go under regular health checks, however Nevada holds one of the highest ranks in STD’s in the U.S. In in some countries in Europe such as Sweden, Netherlands, Norway, and Germany.6
STD rates amongst those who practice sex for money or nonmonetary items hold the greatest risks of contracting HIV because they are more eager to engage in sexual activities with multiple partners and substance use.7 It has been difficult to gather statistics on the HIV and STD rates of sex workers due to its illegalization thus this creates a significant barrier to help target HIV prevention efforts.7 By legalizing prostitution, not only can transmission of HIV be greatly cut down, but the establishment of legal, organized brothels will keep record of every customer that pays for services, protecting these women from rape and abuse, that without legalization, will only grow, and continually get worse.8 This leads us to the question and debate of whether or not prostitution should be legal or illegal. Journalist Paul Armentano cites, “According to current evidence, roughly half of the street prostitutes in Washington, D.C., and New York City are HIV-positive. In Newark, New Jersey, the estimate is that close to 60% of all prostitutes carry the AIDS virus. Yet, in the relatively “free market” of Nevada, where prostitution is legal, not one (as of 1989) of the state-licensed prostitutes has ever tested positive for AIDS nor are they allowed to work as licensed prostitutes.9 During every sexual encounter, the use of condoms is required which is necessary for the semi-guaranteed prevention of unwanted pregnancy and transmission of any sexually categorized disease or infection. Because Nevada’s brothels are regulated, the state licensed prostitutes are required to give monthly blood tests, and each customer that comes to buy sex must fill out health forms . and get physically examined by the company doctor. According to a Public Health article Written by Sally Howard, a UK journalists, she makes note that sex workers face health challenges. Due to fear of authorities and chaotic living patterns it creates a barrier to access healthcare.10
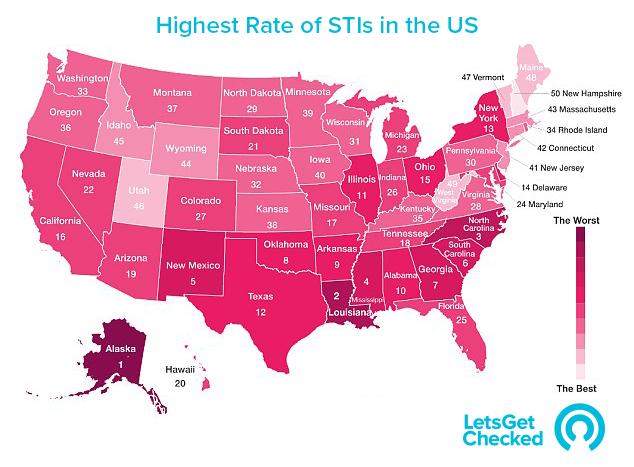 United States, with the highest STD rates have two things in common and that is a lack of appropriate sex education for adolescents and young people, and conservative political views. According to a health testing site called Let’s get checked, states including Alaska and Texas have seen a recent outbreak of chlamydia In Figure 2, we see that Alaska has the heighted rates of STD, whilst New Hampshire come in last place.11 In high schools and states like New Hampshire, where safe sex and STD awareness is being taught in schools, reported the lowest rate of diseases and unplanned pregnancies at just under 16 births per 1,000 girls.11 According to the CDC adolescents and young people aged between 15 to 24 years account for 62.6% of those diagnosed with chlamydia, 52% with gonorrhea which was highly prevalent in the south. Looking at Figure 2, we can also see that the other 10 states with the highest STD ratings either live in a conservative climate or the south, areas where abstinence learning is prevalent.12
United States, with the highest STD rates have two things in common and that is a lack of appropriate sex education for adolescents and young people, and conservative political views. According to a health testing site called Let’s get checked, states including Alaska and Texas have seen a recent outbreak of chlamydia In Figure 2, we see that Alaska has the heighted rates of STD, whilst New Hampshire come in last place.11 In high schools and states like New Hampshire, where safe sex and STD awareness is being taught in schools, reported the lowest rate of diseases and unplanned pregnancies at just under 16 births per 1,000 girls.11 According to the CDC adolescents and young people aged between 15 to 24 years account for 62.6% of those diagnosed with chlamydia, 52% with gonorrhea which was highly prevalent in the south. Looking at Figure 2, we can also see that the other 10 states with the highest STD ratings either live in a conservative climate or the south, areas where abstinence learning is prevalent.12
Figure 2: This map of the United States designed to show the rate of STIS in each state, along with its ranking. The lighter shade represents the states with the lowest rate of STI’s and the darker shades represents an increase in the rate of STIs
Next is the topic of how contraceptive usage such as condoms is impacted by religion , low educational background (which is often associated with low Socioeconomic status), and tradition. Several studies have shown that Sub-Saharan Africa accounted for 68% of global HIV infections, 68% of new adult HIV infections, 92% of new infections in children and 72% of all AIDS-related deaths.13 In a study conducted on youths in Kenya, misinformation and myths were the dominant messages in nearly 46% of communities, and in 33% of communities condoms were described as safe and acceptable only for adults.14 Living in a Catholic and protestant community, it was reported by two-thirds young adults in Zambia that the use of condoms promoted promiscuity. It was also recorded that 54.4% of those who did not use male condoms were from high poverty wards.15
When it comes to religion, according to a study done on infections associated with religious rituals, there was a reporting on an ultra-Orthodox Jewish practice known as Metzitzah b’peh which consists of a ritualistic circumcision on an 8-day old baby. This ritual is practiced amongst 60-90% of the Jewish population in the U.S. .16 Even though, it has been noted by the CDC that men who are circumcised are less likely to contract HIV, herpes and human papillomavirus (HPV), there have been reported cases of at least 22 babies with the herpes simplex virus (HSV) type 1 since the practiced was used.17 The practice is done by a mohel, during the metzitzah the mohel sips wine and then applies his lips to the infant’s genitalia. Failure to perform this act can lead to being barred from performing future circumcisions.16 It can be inferred that a mohel performs these rituals to maintain his status or maybe ignorant to the fact that he is carrying an infectious disease. There has been some type of “preventative” measures implemented which is not specifically said to reduce/stop the infection between mohel and neonate. In the 19th century it is said that Rabbi Moses Schreiber ruled that an instrument such as a glass pipet could be used as a form of protection. This lead to the abandon of suction in favor of a more sterile suction device.16 However some Mohelims have disregarded this alternative. In New . A law in January 2013 has been implemented in New York City for Mohelims to produce consent by the child’s parents for practice. The culture of maintaining a reputation or status can be putting infants at risks. There has been a concern that hospitals are not reporting the cases of 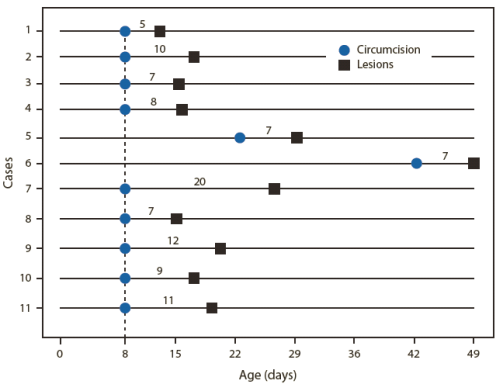 neonatal herpes due to the fear of losing their Hasidic patients.
neonatal herpes due to the fear of losing their Hasidic patients.
Figure 3: Representation of the number of days between Jewish ritual circumcision and appearance of herpes lesions among male infants with neonatal herpes after performance of the Jewish ritual Metzitzah B’peh. The blue circle lines up and represents the age(days) of the neonate, indicating when the procedure was performed. The black squares are plotted on the age(day) the herpes lesions appeared.18
The largest case series has been ported by the Center for Disease Control (CDC)in which they highlighted 11 cases of infants contracting HSV-1 after confirmed or probable oral-genital suction from 2000 to 2011. An investigation was prompted after by NYC Health Department in which they set up a surveillance that uncovered 8 more cases.16 Figure 3 consists of a timeline of all 11 patients documented in NYC. We see that in all but the 5th and 6th cases, both babies were circumcised about 22 and 42 days in age respectively. All the neonates developed 5-11 days after the circumcision was performed.18
There has also been some speculation when it comes to a common practice found in Christianity known as the Holy Communion . This involves the breaking of bread by priest, pastor or minister in honor of Jesus Christ. It has been said that infections can stem from the sharing of the chalice which is used to hold the wine . The CDC has yet to report any data on this but still acknowledges that this is a controversial topic. There has been worry of infections such as Hepatitis B to infect another person but for them to be infected one first must have an open lesion within the oral cavity and would have to be susceptible. Because the communion cup (also referred to as a Chalice) is often wiped with a cloth, the bacteria on it diminishes by about 90%.19 Thus making it hard to detect whether it is a primary effect in transmitting STIs.
Almost every culture comes with its own stigma towards HIV/AIDs and/or other STIs and STDs in all.
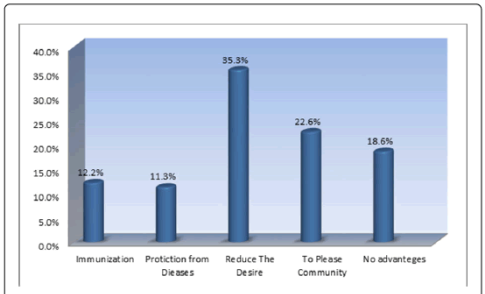
Tradition plays a role in the spreading of STI’s as well. In many countries in Africa and the Middle East, a practice known as Female Genital Mutilation (FGM) is performed on young girls, specifically before they hit puberty. In Figure 4 we see that 35.3% and 22.6% respectively are not in favor of benefits for the woman. But rather, to reduce the desire and please the community.20 Studies have shown that through the sharing of tools and unsanitary conditions STIs such as HIV can spread. Pelvic Inflammatory disease (PID) often occurs as a complication of a STD .21 It was recorded that this complication was noted as a worldwide problem in some countries in Africa, 22% to f44% of women for gynecological problems had PID.21 Most of these women ranging from ages 20-29 years old shared common organisms such as Neisseria gonorrhea and Chlamydia trachomatis.21 This disease was reported three times more prevalent in infibulated women. When it comes to the transmission of HIIV there is rarely any reported linkage between it and FGM. However, there has been
Figure 4: Representation of the advantages in Female Genital Mutilation from men and women20
of these women ranging from ages 20-29 years old shared common organisms such as Neisseria gonorrhea and Chlamydia trachomatis .21 This disease was reported three times more prevalent in infibulated women. When it comes to the transmission of HIIV there is rarely any reported linkage between it and FGM. However, there has been an incident in where a 14-year-old girl from a Malawian tribe was a virgin and 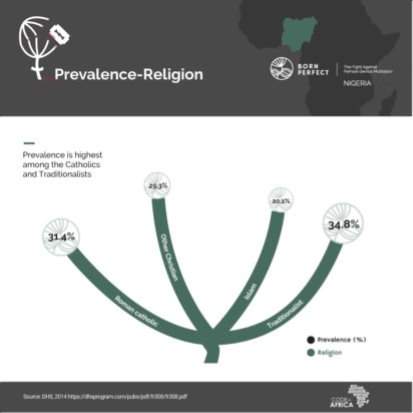 diagnosed as HIV-positive. Inferences have been made that during the tribal circumcision the same blade that was used on several other girls was later used on that 14-year-old girl at the same time.21 Religion, again comes in and plays a role in the action of these practices. In Figure 5, we can see that not only does tradition influence these factors but also many of Roman Catholic church (31.4%), Other Christian church (29.3%) and Islam (20.3%). But we still see that prevalence is highest amongst the Roman catholic and Traditionalists.22 Additionally, due to damage to the female sexual organs, sexual intercourse can result in the laceration of tissue, which greatly increases risk of HIV transmission.21 Statistics also shows that children who have mothers with any educational background are less likely to be cut.23 There have been many programs implemented to stop the practice of Female Genital Mutilation. The number of girls undergoing this process has decreased significantly. The prevalence decreased from 71.4% in 1995 to 8.0% in 2016 in East Africa. In North Africa, the prevalence decreased from 57.7% in 1990 to 14.1% in 2015. In West Africa, the prevalence decreased from 73.6% in 1996 to 25.4% in 2017.24,25 Through this we can see that the implementation of global organizations such as the World Health Organization and UNICEF have impacted these countries governments into putting out a law to protect these women and young girls. Needless to say, the placing a ban has not completely ended the practice. Many rural areas around the world still practice FGM.
diagnosed as HIV-positive. Inferences have been made that during the tribal circumcision the same blade that was used on several other girls was later used on that 14-year-old girl at the same time.21 Religion, again comes in and plays a role in the action of these practices. In Figure 5, we can see that not only does tradition influence these factors but also many of Roman Catholic church (31.4%), Other Christian church (29.3%) and Islam (20.3%). But we still see that prevalence is highest amongst the Roman catholic and Traditionalists.22 Additionally, due to damage to the female sexual organs, sexual intercourse can result in the laceration of tissue, which greatly increases risk of HIV transmission.21 Statistics also shows that children who have mothers with any educational background are less likely to be cut.23 There have been many programs implemented to stop the practice of Female Genital Mutilation. The number of girls undergoing this process has decreased significantly. The prevalence decreased from 71.4% in 1995 to 8.0% in 2016 in East Africa. In North Africa, the prevalence decreased from 57.7% in 1990 to 14.1% in 2015. In West Africa, the prevalence decreased from 73.6% in 1996 to 25.4% in 2017.24,25 Through this we can see that the implementation of global organizations such as the World Health Organization and UNICEF have impacted these countries governments into putting out a law to protect these women and young girls. Needless to say, the placing a ban has not completely ended the practice. Many rural areas around the world still practice FGM.
Figure 5 Prevalence of FGM in Roman catholic, Other Christian, Islam and Traditionalist groups22
DISCUSSION & CONCLUSION
It is without doubt that sexual education has been taught in the United States since the 1960s. However, it has been taught differently throughout the region and around the world as well. Religion and traditional practices has also lead to the hindering of sexual education. We see that Schools that teach abstinence only and tells their students that the only way to avoid contracting an STD/STI or even unwanted pregnancies have higher number of STD/STI or even unwanted pregnancies. In contrast to schools that teach comprehensive sex, we often see the opposite which is less STI’s and unwanted pregnancies.
While preforming this research, one can conclude that the culture has an impact on how individuals view sex and the risks that come a long with it. Sexual education plays a vital role towards these beliefs. A lackluster teaching of what sex is, and the many sexual transmitted disease and infections that can come about it, is doing more harm than good. Young adults who are more likely to engage in risky sexual behavior such as having unprotected sex need to be informed thoroughly about the danger they may be putting themselves in. While observing the study between the Malagasy university and a university in the United States, we see that each group have their own beliefs but one thing that stood out was the difference about sexual education amongst the two groups even though, it is not evident on what type of sex education the students in the U.S received.
When it comes to religion everyone has their own way of serving the God or gods that they worship. But when it comes to a point where humans can have developed a STI then a problem arises. We could observe the negative effects of certain practices in both Judaism and Christianity. When it came to this topic there was prevalent but very limited documentation on incidents such that the infection of genital herpes on eight day old babies and contracting herpes from a communion cup. There has since been no reported incident on babies contracting genital herpes from the practice known as “metzitzah b’peh” as of 2018. We can infer that this is due to the introducing of surveillance. The same thing applies for FGM, the implementing of worldwide organizations and government enforcement has helped to educate many and limit this practice that scars women for life. As for the use of condoms, it is up to priest and other traditional leaders to educte their members on the use of condoms t oboth males and females
The culture of shaming willing sex workers such as prostitutes seems to be leading to an increase of STIs/STDS amongst this group of sex workers rather than banning it completely. In certain countries in Europe where this act has been legalized we see a decrease in STD rates. Perhaps the solution to reducing this act is legalizing it or having some sort of rules and regulations which would result in sex workers going in for mandatory checkups as such..
In all the best thing to combat and change these practices is to educate communities. In the beginning, I introduced a behavioral model for HIV that dealt with biomedical, behavioral and structural interventions. Going into communities even secular ones is very important. Their way of life should be accepted but if it is harming the future and human rights , then government health systems and sexual education must be put into place.
References
- Tannahill, Reay. Sex in History. Stein & Day Pub (July 1, 1982)
- Post MT. Female genital mutilation and the risk of HIV. Washington, DC: Academy for Educational Development, support for Analysis and Research in Africa, 1995;1-10.
- https://www.cdc.gov/hiv/group/sexworkers.html
- https://ac.els-cdn.com/S1201971213001872/1-s2.0-S1201971213001872-main.pdf?_tid=7fd31769-4d53-4731-90e9-e8d6da99b447&acdnat=1544405205_aca12d88410a54ce95dc922db53d3f9d
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4552148/
- Mathieson, Ane; Branam, Easton; and Noble, Anya (2016) “Prostitution Policy: Legalization, Decriminalization and the Nordic Model,” Seattle Journal for Social Justice: Vol. 14 : Iss. 2 , Article 10.
- “HIV/AIDS.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 21 Sept. 2018, www.cdc.gov/hiv/group/sexworkers.html.
- “SiOWfa14 Science in Our World: Certainty and Cont.” SiOWfa15 Science in Our World Certainty and Controversy, sites.psu.edu/siowfa14/2014/10/24/11307/.
- Armentano, Paul. “The Case for Legalized Prostitution.” The Future of Freedom Foundation, 29 Oct. 2012, www.fff.org/explore-freedom/article/case-legalized-prostitution/.
- Howard Sally. Better health for sex workers: which legal model causes least harm? BMJ 2018; 361 :k2609
- Dorff, Gerald J. (1980) “Risk of the Common Communion Cup,” The Linacre Quarterly: Vol. 47: No. 4, Article 7. Available at: http://epublications.marquette.edu/lnq/vol47/iss4/7
- “Sexually Transmitted Disease Surveillance 2017.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 24 July 2018, www.cdc.gov/std/stats17/chlamydia.htm.
- UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. 2010. http://data.unaids.org/pub/Report/2009/JC1700_Epi_Update_2009_en.pdf
- Maticka-Tyndale, & Tenkorang. (2010). A multi-level model of condom use among male and female upper primary school students in Nyanza, Kenya. Social Science & Medicine, 71(3), 616-625.
-
Why don’t urban youth in Zambia use condoms? The influence of gender and marriage on non-use of male condoms among young adults
Pinchoff J, Boyer CB, Mutombo N, Chowdhuri RN, Ngo TD (2017) Why don’t urban youth in Zambia use condoms? The influence of gender and marriage on non-use of male condoms among young adults. PLOS ONE 12(3): e0172062. https://doi.org/10.1371/journal.pone.0172062 - Pellerin, & Edmond. (2013). Infections associated with religious rituals. International Journal of Infectious Diseases, 17(11), E945-E948.
- https://wwwn.cdc.gov/hivrisk/decreased_risk/male_circumcision.html
- Dorff, Gerald J. (1980) “Risk of the Common Communion Cup,” The Linacre Quarterly: Vol. 47: No. 4, Article 7. Available at:http://epublications.marquette.edu/lnq/vol47/iss4/7
- Dorff, Gerald J. (1980) “Risk of the Common Communion Cup,” The Linacre Quarterly: Vol. 47: No. 4, Article 7. Available at:http://epublications.marquette.edu/lnq/vol47/iss4/7
- Ismail KS, Fadol EA, Sheikh ES, Mohammed HA, Elkheir HA, et al. (2017) The Opinion and Role of Men in Female Circumcision in Khartoum State in 2015-2016. Reprod Syst Sex Disord 6: 212. doi:10.4172/2161-038X.1000212
- Brady M. Female genital mutilation: complications and risk of HIV transmission. Aids Patient Care STDS 1999;13(12):709-16.
- Vanguard. “Female Genital Mutilation: Everlasting Cut.” Vanguard News, Vanguard News, 20 Mar. 2018, www.vanguardngr.com/2018/03/we-were-scarred-for-life-before-we-turned-15/.
- “Female Genital Mutilation (FGM) Frequently Asked Questions.” United Nations Population Fund, www.unfpa.org/resources/female-genital-mutilation-fgm-frequently-asked-questions.
- “Data in New Wallchart Show Female Genital Mutilation/Cutting Declining in Many Countries.” Population Reference Bureau, www.prb.org/wallchart-female-genital-mutilation-declining/.
- 1. Kandala N, Ezejimofor MC, Uthman OA, et al. Secular trends in the prevalence of female genital mutilation/cutting among girls: a systematic analysis . BMJ Global Health 2018;3:e000549.
Cite This Work
To export a reference to this article please select a referencing style below:
Related Content
All TagsContent relating to: "STI"
Sexually transmitted infections affect people of all ages with the greatest occurrence amongst those under the age of 25 years. In the UK, certain groups of populations are affected more than others thus creating sexual health inequalities.
Related Articles
