
Case profile
The client:
Tim* was a ten-year-old male with no formal diagnosis.
Previous relevant medical history:
Tim was born at 35 weeks and remained in intensive care for six months post birth. This is relevant as a pre-term birth increases the risk of delayed neurodevelopment (Schieve et al., 2016) with a recent study also suggesting that functional limitations in activities of daily living (ADLs) “do not appear to self-correct and could lead to poorer educational attainment” (Killeen et al., 2014, p.304) in children who were born pre-term.
There are no other aspects from the details provided of Tim’s medical history which were relevant to the occupational therapy process.
Family status:
Tim was an only child. Tim’s mother was on leave from her job as a nurse as she was undergoing treatment for early stage breast cancer of which the prognosis was quite positive (Harbeck and Gnant, 2017), however this did cause Tim’s mother acute fatigue. Tim’s father was employed on a full-time basis by a local construction company. The family was not in receipt of formal support within the home at the time. Tim often was required to assist in the running of the home, e.g. completing household chores.
School:
Tim attended a local primary school with fewer than forty children in attendance overall. Tim’s mother noted in the referral form that Tim did not receive formal support within the school, e.g. resource hours, however, as the class was small, the class teacher was able to provide Tim with increased assistance as required.
Leisure:
Tim enjoyed playing football after school with the local club and travelled to training with a friend who lived nearby however he often missed football training due to time spent completing homework tasks. Tim also enjoyed drawing pictures.
Reason for referral to occupational therapy:
After discussion with Tim’s parent’s and with their informed consent, the class teacher referred Tim to occupational therapy. The class teacher identified concerns relating to Tim’s motor skill development and handwriting ability.
Parental concerns as identified on the referral form (in order of priority):
- Tim’s handwriting was illegible and his speed of production was very slow. This was preventing him from participating adequately in class activities which he enjoyed, e.g. story writing.
- Tim was unable to tie the small buttons on his school shirt.
- Tim had difficulty completing drawing tasks, which he enjoyed, due to hand fatigue.
Model of Practice
The model of practice chosen was the Person – Environment – Occupation and Performance model (PEOP, Baum, Bass-Haugen and Christiansen, 2005). The PEOP model is a client-centered model, which links with current occupational therapy practice guidelines outlined in the Occupational Therapists Registration Board Code of Professional Conduct and Ethics Bye-law 2014 that emphasise client-centred practice as central to occupational therapy. However, in the context of the approach to Tim’s care, “family-centred care, which recognizes the importance of including the family in a child’s care [and] is currently the most well-established approach to health service delivery for children” (Hayles et al., 2015, p.1) must also be applied, which using the PEOP allows for, due to the model’s design (Lee, 2010). The model also considers the family, which in Tim’s case is a hugely influencing factor on the occupational therapy process and how they can act as facilitators or barriers to Tim’s occupational performance (Baum, Bass-Haugen and Christiansen, 2005).
A primary reason for choosing the PEOP model was that it allowed for service requirements to be met whilst ensuring that the therapist maintained an occupational perspective (Joosten, 2015, p.221). Models such as the Model of Human Occupation (MOHO, Kielhofner, 2008) are process-based and are based upon the theory that changing a client’s intrinsic factors will cause an improvement in occupational engagement (Wong and Fisher, 2015). The PEOP model is a ‘top-down’ model but it also allows for analysis of the underlying factors (i.e. person factors and environment factors) which contributed to the limitations in occupational participation (Wong and Fisher, 2015); thus enhancing the therapist’s knowledge of the nature of the occupational problem, whilst also allowing the occupational therapist to adhere to service requirements which dictated a need for the assessment of performance components. The occupational therapist could then apply the knowledge of the performance components, e.g. Tim’s in-hand manipulation skills, to enrich the therapists overall image of the context of Tim’s participation in occupation. This subsequently allowed for occupation-focused goals to be collaboratively set with the client.
Initial assessment
| Location of assessment: A quiet, distraction-free room within the service. Chair and table supplied to Tim were like those used in Tim’s classroom at school. | |
| People present: Tim, Tim’s father and the occupational therapist. | |
| Behaviour during assessment: Tim was polite, well-mannered and motivated to engage, even with tasks he found difficult. Tim was eager to please and followed instructions as asked. He maintained adequate concentration for the duration of the assessment but did pause frequently to stretch his hands, reporting that they were “tired”, which increased the testing period considerably. | |
| Description | Results/ interpretation |
| Prior to conducting the initial assessment session (as Tim did not have a case file available to the service or input from other members of the multi-disciplinary team) a phone call was made to Tim’s father to elaborate on the concerns noted in the referral form. | He reported that the concerns listed were still accurate and that him or his wife had no concerns regarding Tim’s performance in social occupations, self-care occupations or Tim’s performance in activities requiring gross-motor skills. Tim’s father reported that Tim’s mother was currently quite unwell and would not be able to participate in the occupational therapy process at present.
Tim’s father reported that as Tim’s mother was ill and he worked late in the evening, Tim often completed household tasks such as washing the dishes or doing the laundry but that he had not practice handwriting tasks supervised at home over the past year. Tim’s father also stated that Tim could be completing homework until he returned from work, approximately four hours after Tim would begin his homework. This worried Tim’s father as Tim often missed football training, an important source of social support and leisure (Baum, Bass-Haugen and Christiansen, 2005) to Tim during the emotionally difficult period imposed by his mother’s illness. Tim confirmed this later during the initial assessment session and stated he did so as he did not want to get in trouble in school for not having his homework completed. Tim’s father gave informed consent to ring the class teacher for discussion regarding Tim’s school performance. |
| Assessment of Tim’s handwriting speed using a standardized assessment called the ‘Detailed Assessment of Speed of Handwriting’ (DASH, Barnett, Henderson, Scheib and Schulz, 2007) was conducted.
Rationale: The DASH was a comprehensive measure of a child’s handwriting speed which has been standardized and norm-referenced within the United Kingdom (Barnett, Henderson, Scheib and Schulz, 2009). It was reported to have “good to excellent” test-retest reliability, allowing it to be used as an outcome measure for intervention (Francis, Wallen and Bundy, 2016, p.166). It also allowed for direct observation of Tim’s handwriting performance and analysis of the written output. A standardised measure to assess handwriting legibility was not available within the service. Upon consultation with the practice educator, it was agreed that observation and analysis of the written output would allow for richer data collection. |
Speed:
Tim scored at the 35th percentile overall which indicated that speed of handwriting was not a concern. However, Tim’s score in the “copy best” (Barnett, Henderson, Scheib and Schulz, 2007) task was significantly lower than the other subtests as Tim’s speed of approach to this subtest was extremely slow, however, this resulted in the production of Tim’s most legible sample of writing. It is also important to note that illegible words were scored for the “free writing” subtest (Barnett, Henderson, Scheib and Schulz, 2007) and that the sample provided was almost 65% illegible. Tim’s handwriting speed was age-appropriate but the written work completed was illegible and he began to fatigue towards the end of the assessment (approximately twenty minutes) which suggests that poor handwriting endurance may be the primary factor for reduced handwriting speed over a period of time. Legibility: Tim wrote using script as this is what was taught in school. The sizing of Tim’s handwriting was inconsistent, with inadequate letter proportion being a significant issue. Slant was not identified as an issue. Letters were often over 1cm above or below the lines. Spacing between words or letters was adequate. Tim’s fine-motor skills appeared to be adequate. Letter formation was inadequate, with Tim often beginning letters in the incorrect starting position. Tim’s writing endurance was poor with legibility significantly decreasing as the assessment progressed. Tim’s literacy skills were adequate. Pencil grip was not assessed as research has disproved the hypothesis that handwriting legibility is impacted by the type of pencil grip (Dennis and Swinth, 2001). Tim’s overall handwriting legibility was impacted most by poor handwriting endurance and difficulties with the sizing of letters, placement on the line and beginning letters in the correct position. |
| Observation of Tim buttoning and unbuttoning the top three buttons of his school shirt. | Tim was observed to have difficulty fastening and unbuttoning the buttons of his school shirt. Tim could grasp the seam of the shirt with his left hand and manipulate the buttons adequately with his index finger and thumb. However, he was very slow to complete the task.
Tim’s dad stated that he often was delayed going to work as Tim needed him to be there to button his school shirt as it took Tim a considerably long period of time to complete. |
| Observation of Tim completing a “connect-the-dots” drawing task. As Tim enjoyed these types of tasks he engaged readily and it provided an opportunity for direct observation of Tim’s fine-motor co-ordination and control, visual-motor integration and endurance. | Tim completed this task adequately but complained of hand fatigue towards the end of the task. No difficulties were observed with fine-motor control or visual-motor integration. |
| Phone-call to Tim’s class teacher. | The teacher reported that Tim’s handwriting had become progressively more illegible over the past year and that it took him a long period of time and frequent encouragement to produce written work in a timely manner as he often took breaks due to hand fatigue.
As Tim’s work was illegible he often scored poorly in class tasks, but she felt this was not a true reflection of his abilities. |
Occupational problems
The therapist met with Tim’s father to discuss the results of the assessment and prioritise occupational problems.
Occupational problems:
- Tim’s written work was 65% illegible which resulted in reduced performance of class tasks which were not reflective of his cognitive ability (Baum, Bass-Haugen and Christiansen, 2005).
- Tim could not sustain handwriting for an adequate period to complete his homework in a reasonable period of time, often spending up to four hours per night. This prevented Tim participating in football training.
- Tim could not button or unbutton his school shirt in a timely manner, which resulted in disruption of his father’s daily routine also.
Occupational strengths:
- Tim was motivated to participate in all classroom tasks and always tries his best to complete his homework independently.
- Tim can dress himself independently, except for buttoning his school shirt.
- Tim could complete age-appropriate household tasks independently.
Goals of Intervention
The PEOP model (Baum, Bass-Haugen and Christiansen, 2005) does not prescribe interventions but emphasizes that goals for intervention must be occupation-based, i.e. ‘top-down’, and reflect the client’s unique occupational context (Baum, Bass-Haugen and Christiansen, 2005; Joosten, 2015). Tim’s goals were set collaboratively with Tim’s father, the therapist and the classroom teacher. The therapist identified that handwriting remediation required repetitive task-orientated practice (Hoy, Egan and Feder, 2011) but that as Tim’s parents were not able to contribute time to this at present, the class teacher may have been able to collaborate with the occupational therapist to deliver parts of the intervention whilst Tim’s mother was ill. Each person present contributed to setting goals and identifying how to navigate the barriers to Tim’s participation which were identified during the assessment.
Goal: By the end of the term, Tim’s writing during class tasks would be under 40% illegible.
Rationale: Tim’s illegible handwriting was reducing his overall performance in class tasks, which did not reflect his abilities in other aspects of learning.
Steps to achieve this: Task-specific practice under the supervision of the class teacher, focusing on handwriting tasks which aim to remediate letter sizing, placement on the line and the correct starting position of letters. Tim will be allowed to complete these additional tasks whilst the rest of the class are completing free-writing tasks. Homework for the weekend will relate to this intervention, which Tim’s father will supervise.
Goal: By the end of the week, Tim would be able to complete his homework within one hour.
Rationale: Tim’s homework was taking him too long and resulting in an occupational imbalance (Anaby et al., 2010) and although Tim’s poor writing endurance was impacting on classroom tasks also, homework was prioritized as Tim’s father was concerned that it was impacting on Tim’s leisure and social occupations during an emotionally difficult time for the family.
Steps to achieve this: Tim’s teacher agreed that one-hour was an appropriate length of time and she will explain to Tim that he may stop homework after one hour, regardless of if it is completed. If Tim does not have a sufficient amount completed, she will assist Tim in prioritising homework tasks before he leaves school. Tim’s parents would report to the teacher if they observed Tim spending over one hour per day.
Goal: Tim would be able to button his school shirt independently by the last day of the school term.
Rationale: This was the only aspect of dressing which Tim could not complete independently in the morning due to time constraints. If Tim learnt this age-appropriate skill it would improve the family’s morning routine and increase Tim’s occupational performance and independence.
Steps to achieve this: The therapist conducted an activity analysis of the task of buttoning and unbuttoning the school shirt and used this to analyse how to instruct Tim’s father to grade the activity to gradually increase Tim’s participation in the task. As Tim’s parents did not have time to practice buttoning during the weekdays, a graded approach will be used midweek based upon the therapist’s activity analysis, and repetitive practice will be emphasised at the weekends when Tim’s father has time to supervise this.
Search strategy
The PICO used:
Person – Child between the ages of five years and eighteen years old.
Intervention – A task-orientated approach to improving handwriting legibility.
Comparison – Process-based approaches to improving handwriting legibility/
Outcome – The child’s handwriting legibility improves.
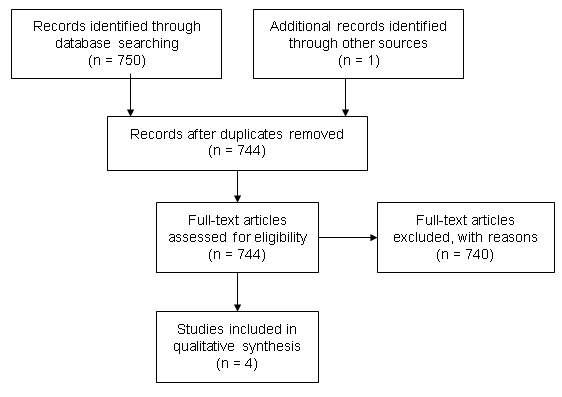
The database search:
Three databases were searched: The Cochrane Library, OTSeeker and Scopus. One article was also identified through hand-searching of the reference lists of three articles. The following keywords ‘handwriting’, ‘intervention’, ‘therapy’, ‘approach’, ‘treatment’, ‘program’, ‘programme’, ‘paediatric’, ‘children’, ‘students’ and ‘child’ were used and Boolean logic applied (see Appendix 1.0). Minor adjustments to the formatting of the Boolean logic applied, e.g. use of brackets, was required depending on the database searched. The terms ‘task-orientated’ or ‘legibility’ were not included in the search strategy as they caused the results to be over-limited; excluding these terms increased the likelihood of a comprehensive search of the literature.
Inclusion/ exclusion criteria:
Inclusion criteria applied was 1) that handwriting intervention was provided to participants, 2) that participants were aged between five years of age (as handwriting is not taught until primary school) and eighteen years of age, 3) the intervention was not specific to a diagnosis, e.g. developmental co-ordination disorder, 4) a task-orientated approach to handwriting was investigated and 5) handwriting legibility was included as an outcome measure. Exclusion criteria applied was 1) if the inclusion criteria above were not met, 2) if the full text was not available freely through the university or HSE as funding for the purchase of articles was not available, 3) if the article was not available in the English language as funding for translation of articles was not available or 4) the intervention was not specific to a diagnosis, e.g. developmental co-ordination disorder.
Articles chosen:
The articles were screened initially from full text for suitability and assessed for eligibility as per the inclusion and exclusion criteria identified (see Appendix 1.1 and Appendix 1.2). The decision was made not to screen from abstract initially as many articles did not outline legibility as a primary outcome reported in the abstract. A total of five studies were included in the final review (see Appendix 1.3) with one article outlining two studies conducted (Jongmans, Linthorst-Bakker, Westenberg and Smits-Engelsman, 2003).
Critical appraisal of literature
The Critical Appraisal Skills Program (CASP, Critical Appraisal Skills Programme, 2017) forms were used to review methodological quality of the studies and classify them into levels of evidence (see Appendix 1.4).
The systematic review by Hoy, Egan and Feder (2011) titled “A Systematic Review of Interventions to Improve Handwriting” was of the highest evidence (i.e. Level I). It critiqued eleven articles of which nine were randomized controlled trials and the other two, controlled trials. The review concluded that repetitive handwriting practice is the most effective intervention to improve written output in school-aged children and that handwriting intervention provided by occupational therapists should emphasise task-orientated handwriting practice and avoid bottom-up approaches which are reported to be ineffective authors (Hoy, Egan and Feder, 2011). Factors identified which increase the validity and reliability of the systematic review by Hoy, Egan and Feder (2011) addressed a clear question, i.e. ‘what handwriting interventions which could be used by occupational therapists are most effective in improving written output amongst school-aged children?’, searched for controlled trials only as this type of study is most appropriate for evaluating interventions, searched all major databases increasing the chances of a comprehensive search and two authors critiqued the literature sourced and compiled the results of the review independently to reduce bias. By focusing the review on school-aged children, the results are more generalizable to the client. Limitations of the review include that articles not published in the French or English language were discarded increasing the chances of missed literature, details of the author’s critique of each article’s methodological quality was not detailed in the study which limits the reliability of the study. Also, many of the studies included in the review had small sample sizes although this was identified as a limitation by the authors (Hoy, Egan and Feder, 2011). Overall, although this study appears to have adequate methodological quality to apply the results of the review to the client, the lack of information regarding the authors critique of the individual studies rigour indicates that the results must be interpreted with caution.
The randomized controlled trial titled “Use of a task-oriented self-instruction method to support children in primary school with poor handwriting quality and speed” by Zwicker and Hadwin (2009) compared two occupational therapy interventions to improve handwriting legibility in seventy-three primary-school aged children; cognitive intervention (which directly relates to a task-orientated approach as it emphasises direct practice of the task as opposed to remediation of process-based skills) and multi-sensory based intervention. Each child (except those in the control group) received one thirty-minute individual occupational therapy session each week for ten weeks (Zwicker and Hadwin, 2009). The results highlighted that the cognitive approach was more effective at improving handwriting legibility than the multi-sensory approach, with no notable change in the scores of the control group (Zwicker and Hadwin, 2009). No statistically significant change was detected for either group, however handwriting legibility improved for all participants in the cognitive group compared with the multisensory and control group where 4 out of 9 and 3 out of 10 participants respectively, were identified to have worsened handwriting legibility. Limitations of this study included the lack of blinding and the use of convenience sampling which increased the risk of bias, the fact that the sample was obtained from one school in America decreased the generalisability of this study to the client.
The article “Cognitive versus Multisensory Approaches to Handwriting Intervention: A Randomized Controlled Trial” by Jongmans, Linthorst-Bakker, Westenberg and Smits-Engelsman (2003) outlined two studies, one in a mainstream primary school (Study 1) and the second in a special education school (Study 2) and a control group. The studies aimed to identify if a self-instruction approach could improve handwriting quality (including legibility) and handwriting speed (Jongmans, Linthorst-Bakker, Westenberg and Smits-Engelsman, 2003). The intervention varied in delivery method between the two studies, i.e. study 1 was delivered via individual sessions, twice a week, over the course of three months as opposed to group sessions, twice a week over six months in study 2, and in design, i.e. study 1 was a pre-post-test design whereas study 2 was a quasi-experimental case-control design (Jongmans, Linthorst-Bakker, Westenberg and Smits-Engelsman, 2003). The intervention sessions are poorly described which poses a threat to both the validity and genarilisability of the study as the intervention provided cannot be critiqued or easily replicated. It was decided to discontinue the critique of this study at this point as the rigour of the study was poor and therefore not applicable to this case (Critical Appraisal Skills Programme, 2017).
The final article “Assessing Handwriting Intervention Effectiveness in Elementary School Students: A Two-Group Controlled Study” by Howe, Roston, Sheu and Hinojosa (2012). This article compared the effectiveness of two handwriting interventions, “intensive handwriting practice and visual–perceptual–motor activities” (Howe, Roston, Sheu and Hinojosa, 2012, p.19), in improving handwriting legibility and speed amongst a cohort of primary school children. Participants were assigned to either an intensive practice group or a visual-perceptual-motor group and intervention was delivered in group settings over forty-five minutes, two times a week for six weeks, with a pre-post-test design applied (Howe, Roston, Sheu and Hinojosa, 2012). Standardised assessments of handwriting legibility, speed and visual-motor integration were used as outcome measures to reduce the risk of bias. Whilst the results of the study indicated that intensive practice was the more effective intervention, there were many study limitations which reduce the validity, reliability and generalisability of the study such as no attempt to control for confounding factors, a small sample size (n = 72), only one scorer for the standardised assessments and the geographical location of the study (i.e. New York, United States of America).
Overall, whilst all studies included conclude that a task-orientated approach to handwriting intervention is more effective than a process-based approach, the methodological quality of the studies critiqued are open to numerous threats to internal validity, decreasing the reliability and generalisability of the studies. However, the systematic review by Hoy, Egan and Feder (2011) appeared to have the most rigorous methodology and was of the highest evidence of the studies found, therefore the results of this study, which indicate a task-based approach be used, will be applied to Tim’s case.
Discussion of application of evidence to case study
The evidence suggested that frequent practice of handwriting specific tasks, not activities which aim to remediate components of handwriting, e.g. muscle strength, are more effective at improving the legibility of written output for primary school children like Tim who do not have a formal diagnosis (Hoy, Egan and Feder, 2011). The practice setting demands allowed for just one intervention session and one review session to occur as Tim was not high enough on the priority list, therefore supervision of the intervention sessions could not be facilitated by the therapist as per the studies reviewed. However, due to the difficult family circumstances, facilitation by the parents to the recommended frequency was not possible and as Tim’s school had a high teacher to pupil ratio, reasonable accommodations were provided by the class teacher, a professional, to deliver majority of the intervention sessions required.
This intervention also fitted with the principles of the PEOP model (Baum, Bass-Haugen and Christiansen, 2005) best due to it’s top-down approach.
Description of intervention session
Goals being addressed: All prioritised goals were addressed.
Location: Tim’s school in a private and quiet room. This was chosen so that the class teacher could be present and it was closer to Tim’s father’s workplace.
People present: Tim’s father, the class teacher and the therapist. Tim was not present for this session as he was sick that morning and could not attend school. Tim’s father had called the therapist in the morning to advise of this but stated that he would have to meet that day for the session as arranged as he could not take another day off work.
Session objectives and content: To educate Tim’s father and teacher on the aims, procedure and facilitation techniques necessary to deliver the school-/ home- based interventions developed by the therapist to achieve the collaborative goals. The therapist ensured that they understood the rationale for the intervention, it’s principles, how best to facilitate success and how, if or when they should contact the therapist regarding the intervention. The therapist educated the teacher and Tim’s father using a combination of modelling and instruction, which was supplemented with written descriptions, example worksheets and information sheets regarding the school/home based programs. Time was provided for questions and the therapist’s number was provided in case of any future questions.
Treatment approach: Task-specific practice to remediate handwriting difficulties and learning to button the school shirt. A time-limit was applied to homework to reduce the time spent at this occupation.
Frames of reference applied: No person factors were identified during assessment which may impact on the development handwriting or dressing skills and therefore a developmental frame of reference (Murray, 2013) was adopted to meet the first goal of improving Tim’s handwriting skills to increase the legibility of his work and hence improve overall occupational performance in class activities requiring handwriting. It was hypothesised that the high-intensity of handwriting specific task-practice would also improve Tim’s handwriting endurance, which relates to the biomechanical frame of reference (Kramer & Hinojosa, 2009).
A compensatory frame of reference (Murray, 2013) was adopted to meet the homework goal (goal two) as an immediate effect was required to ensure occupational balance whilst handwriting skills were being developed. An educational frame of reference (Murray, 2013) was applied when educating the teacher and Tim’s father on delivering the handwriting intervention and when educating Tim’s father on delivering the buttoning intervention, so that they understood the rationale for the intervention, it’s principles and how best to facilitate success.
Client evaluation of session: The class teacher and Tim’s father reported they understood the information provided, the procedure to be followed and could identify how and when to liaise with the therapist.
Therapist’s evaluation of session: The teacher and Tim’s father participated well in the session, asked questions appropriately and by the end of the session could demonstrate the appropriate skills required to facilitate the school and home program provided.
Evaluation of intervention
The full review session was scheduled for the end of the school term, therefore an evaluation of whether goals were met was not conducted during the placement. This would have consisted of re-administration of the initial assessments conducted. As handwriting speed was not identified as a concern during the initial assessment, a written sample from school could have been used to assess improvements in legibility, however, use of the ‘Detailed Assessment of Speed of Handwriting’ (DASH, Barnett, Henderson, Scheib and Schulz, 2007) would allow for direct observation over the same period and analysis of the same written output.
To review progress of the goals, a phone call was made to Tim’s father at the end of the first week to identify if the homework goal was met. Tim’s father reported that Tim was happy with the arrangement and had not missed any football training since. He stated that Tim initially was not completing math’s homework as he was used to doing this first but that the class teacher had identified this issue and prioritized Tim’s homework at the end of each day to leave handwriting tasks until last as he was already receiving intensive input for this within class. This goal was fully met.
Tim’s father reported also that Tim was focusing on buttoning two buttons independently in the morning before asking for help but that they would be practicing three at the weekend and would hopefully be progressing to this then as per the grading instructions provided by the therapist. This goal was not fully met yet but progress had been identified as Tim was originally not attempting to do up the buttons anymore in the mornings and was again beginning to try with guidance from his father.
To identify if Tim’s handwriting legibility was improving, the therapist made a phone-call to Tim’s class teacher to discuss the intervention sessions being facilitated and identify any concerns. The teacher stated that the intervention was easy to follow and that working on the three aspects of handwriting legibility identified was having a significant impact on the legibility of Tim’s handwriting and subsequently his performance in class tasks and assessments had increased. A work sample was requested which the teacher posted to the therapist, with parental consent, and analysed by the therapist – 40% of words were deemed illegible which indicated an improvement in written output, i.e. occupational performance (Baum, Bass-Haugen and Christiansen, 2005). As a result, the therapist consulted with Tim’s father and class teacher, via phone-call, to adjust the goal to reflect the rapid improvement and a reduction to 30% illegible words as opposed to 40% was collaboratively agreed.
Overall the intervention to date was successful and given the constraints on direct patient contact within the service at the time, collaborating with the school allowed for parts of the intervention delivery to be delivered by a professional who knew Tim well, on a regular basis. However, Tim should have been present for an intervention session to allow for the therapist to explain the intervention to Tim and to provide an opportunity for the class teacher and Tim’s father to practice delivering the school/home programs under supervision initially and receive feedback.
Note: * = Tim is a pseudonym and not the client’s real name.
References
Anaby, D., Jarus, T., Backman, C. and Zumbo, B. (2010) “The Role of Occupational Characteristics and Occupational Imbalance in Explaining Well-being”, Applied Research in Quality of Life, 5(2), pp. 81-104.
Barnett, A., Henderson, S., Scheib, B. and Schulz, J. (2009) “Development and standardization of a new handwriting speed test: The Detailed Assessment of Speed of Handwriting”, British Journal of Educational Psychology, 2(6), pp. 137-157.
Barnett, A., Henderson, S., Scheib, B. and Schulz, J. (2007) The Detailed Assessment of Speed of Handwriting (DASH): Manual. Pearson Education.
Baum, C., Bass-Haugen, J., Christiansen, C.H. (2005) Person, environment, occupation and performance. A model for planning interventions for individuals and organisations. In Christiansen C, Baum C, Haugen J (2005) Occupational therapy: performance, participation and wellbeing (3rd ed). Thorofare: SLACK Inc.
Critical Appraisal Skills Programme (CASP) (2017) Critical Appraisal Skills Programme (CASP). Available at: http://www.casp-uk.net/casp-tools-checklists (Accessed: 12 October 2017).
Dennis, J. and Swinth, Y. (2001) “Pencil Grasp and Children’s Handwriting Legibility During Different-Length Writing Tasks”, American Journal of Occupational Therapy, 55(2), pp. 175-183.
Denton, P., Cope, S. and Moser, C. (2006) “The Effects of Sensorimotor-Based Intervention Versus Therapeutic Practice on Improving Handwriting Performance in 6- to 11-Year-Old Children”, American Journal of Occupational Therapy, 60(1), pp. 16-27.
Feder, K. and Majnemer, A. (2007) “Handwriting development, competency, and intervention”, Developmental Medicine & Child Neurology, 49(4), pp. 312-314.
Francis, A., Wallen, M. and Bundy, A. (2016) “Comparison of the Properties of the Handwriting Speed Test (HST) and Detailed Assessment of Speed of Handwriting (DASH): An Exploratory Study”, Physical & Occupational Therapy in Paediatrics, 37(2), pp. 155-169.
Harbeck, N. and Gnant, M. (2017) “Breast cancer”, The Lancet, 389(10074), pp. 1134-1150.
Hayles, E., Harvey, D., Plummer, D. and Jones, A. (2015) “Parents’ Experiences of Health Care for Their Children with Cerebral Palsy”, Qualitative Health Research, 25(8), pp. 1-16.
Henderson, S.E. and Sugden, D.A. (2007). Movement Assessment Battery for Children.2nd Ed. London: Pearson.
Howe, T., Roston, K., Sheu, C. and Hinojosa, J. (2012) “Assessing Handwriting Intervention Effectiveness in Elementary School Students: A Two-Group Controlled Study”, American Journal of Occupational Therapy, 67(1), pp. 19-26.
Hoy, M., Egan, M. and Feder, K. (2011) “A Systematic Review of Interventions to Improve Handwriting”, Canadian Journal of Occupational Therapy, 78(1), pp. 13-25.
Jongmans, M., Linthorst-Bakker, E., Westenberg, Y. and Smits-Engelsman, B. (2003) “Use of a task-oriented self-instruction method to support children in primary school with poor handwriting quality and speed”, Human Movement Science, 22(4-5), pp. 549-566.
Joosten, A. (2015) “Contemporary occupational therapy: Our occupational therapy models are essential to occupation centred practice”, Australian Occupational Therapy Journal, 62(3), pp. 219-222.
Kielhofner, G. (2008) Model of human occupation. 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 1-6.
Killeen, H., Shiel, A., Law, M., Segurado, R. and O’Donovan, D. (2014) “The impact of preterm birth on participation in childhood occupation”, European Journal of Paediatrics, 174(3), pp. 299-306.
Kramer, P. and Hinojosa, J. (2009). Frames of reference for pediatric occupational therapy (3rd ed.). Baltimore: Lippincott, Williams & Wilkins.
Lee, J. (2010) “Achieving Best Practice: A Review of Evidence Linked to Occupation-Focused Practice Models”, Occupational Therapy in Health Care, 24(3), pp. 206-222.
Medwell, J., Strand, S. and Wray, D. (2007) “The links between handwriting and composing for Y2 children”, Journal of Reading, Writing and Literacy, 2(1), pp. 11-21.
Murray, L., (2013). “Models, Frame of References & Learning Theories”. Mental Health 1. [Online] Available at: https://nuigalway.blackboard.com/webapps/blackboard/execute/content/file?cmd=view&content_id=_621334_1&course_id=_41164_1&framesetWrapped=true. (Accessed 24 October 2017).
Occupational Therapists Registration Board Code of Professional Conduct and Ethics Bye-law 2014 (SI no. 527 of 2014).
Schieve, L., Tian, L., Rankin, K., Kogan, M., Yeargin-Allsopp, M., Visser, S. and Rosenberg, D. (2016) “Population impact of preterm birth and low birth weight on developmental disabilities in US children”, Annals of Epidemiology, 26(4), pp. 267-274.
Schwellnus, H., Carnahan, H., Kushki, A., Polatajko, H., Missiuna, C. and Chau, T. (2012) “Effect of Pencil Grasp on the Speed and Legibility of Handwriting in Children”, American Journal of Occupational Therapy, 66(6), pp. 718-726.
Wong, S. and Fisher, G. (2015) “Comparing and Using Occupation-Focused Models”, Occupational Therapy in Health Care, 29(3), pp. 297-315.
Zwicker, J. and Hadwin, A. (2009) “Cognitive versus Multisensory Approaches to Handwriting Intervention: A Randomized Controlled Trial”, OTJR: Occupation, Participation and Health, 29(1), pp. 40-48.
Bibliography
Burke, P. and Flattery, V. (2010) Professional Supervision in Occupational Therapy. 1st ed. Galway: Association of Occupational Therapists Ireland, pp. 4-24. Available at: https://www.aoti.ie/attachments/9875f756-9a10-46b7-a6b9-b34162611e4b.PDF (Accessed: 5 October 2017).
Appendices
Appendix 1.0 (Search strategy)
| Database | Keywords | Boolean logic |
| Cochrane
OTSeeker Scopus (1 paper was hand searched from the reference list of three articles found during the search) |
Handwriting
Intervention Therapy Approach Treatment Program Programme Paediatric Children Students |
((“handwriting”) AND (“intervention” OR “therapy” OR “approach” OR “treatment” OR “program” OR “programme”) AND (“child” OR “children” OR “students” OR “paediatric”)) |
Note: A task-orientated approach or legibility were not included in the keywords as they caused results returned to be over-limited.
Appendix 1.1
| Name of database | Number of papers found | Number of papers rejected from initial screening |
| Cochrane | 43 | 41 (11 – handwriting intervention not investigated, 30 – Task-orientated approach not included) |
| OTSeeker | 11 | 8 (1 – adults, 6 – Task-orientated approach not included, 1 – handwriting legibility not an outcome) |
| Scopus | 696 | 691 (5 – included adults, 224 – Handwriting intervention not investigated, 438 – Task-orientated approach not included, 8 – handwriting legibility was not an outcome, 18 – Specific to a client condition) |
| Hand searched (3) | 1 | 0 |
Appendix 1.2
| Inclusion criteria | Number of papers rejected | Reasons for rejection (exclusion criteria) |
| Handwriting intervention was provided to participants. | 235 | Handwriting intervention not provided – 235 |
| Participants were aged between five years of age and eighteen years of age. | 6 | Included participants under the age of five – 0
Included participants over 18 years of age – 6 |
| Intervention not specific to a diagnosis, e.g. developmental co-ordination disorder | 18 | Specific to a diagnosis – 18 |
| A task-orientated approach to handwriting was investigated. | 471 | Task orientated approach not investigated – 471 |
| Handwriting legibility was included as an outcome measure. | 10 | Handwriting legibility was not an outcome measure – 10 |
| Full text was available. | 0 | Full text not available – 0 |
| Full text was published in the English language and this version was available. | 0 | English language full text version not available – 0 |
Appendix 1.3 (Prisma)
Appendix 1.4 (Literature selected for review)
| Level of evidence | Number of articles
|
Reference |
| Level I – Evidence from a systematic review or meta-analysis from all relevant RCTs | 1 | Hoy, M., Egan, M. and Feder, K. (2011) “A Systematic Review of Interventions to Improve Handwriting”, Canadian Journal of Occupational Therapy, 78(1), pp. 13-25. |
| Level II – Evidence from at least one well designed RCT | 0 | |
| Level III – Evidence from well-designed controlled trials without randomisation | 2 (1 – Poorly designed RCT
|
Jongmans, M., Linthorst-Bakker, E., Westenberg, Y. and Smits-Engelsman, B. (2003) “Use of a task-oriented self-instruction method to support children in primary school with poor handwriting quality and speed”, Human Movement Science, 22(4-5), pp. 549-566.
Zwicker, J. and Hadwin, A. (2009) “Cognitive versus Multisensory Approaches to Handwriting Intervention: A Randomized Controlled Trial”, OTJR: Occupation, Participation and Health, 29(1), pp. 40-48. |
| Level IV – Evidence from well-designed case-controlled and cohort studies | 1 | Howe, T., Roston, K., Sheu, C. and Hinojosa, J. (2012) “Assessing Handwriting Intervention Effectiveness in Elementary School Students: A Two-Group Controlled Study”, American Journal of Occupational Therapy, 67(1), pp. 19-26. |
| Level V – Evidence from systematic reviews of descriptive and qualitative studies | 0 | |
| Level VI – Evidence from a single descriptive or qualitative study | 0 | |
| Level VII – Evidence from the opinion of authorities and/or reports of expert committees | 0 |
Cite This Work
To export a reference to this article please select a referencing style below: