Reflection on Care Interventions and Decision Making
Info: 4007 words (16 pages) Reflective Nursing Essay
Published: 15th Dec 2020
Tagged: reflective practicecare
Reflective evaluation of care interventions in mental health nursing
Introduction
This essay is a reflective examination of a care episode in the domain of mental health nursing, in relation to the processes of nursing decision making, clinical reasoning, and processes associated with patient care planning and management. The reflection on elements or aspects of care, or on specific clinical experiences, is an important part of nurse development and ongoing professional practice (Rolfe, 2005). Reflection is more than simply looking back at experiences and incidents, it is a process of making sense of them, understanding all the dimensions of an experience, and using information, evaluation and analysis to improve future practice (Hargreaves, 2004). It is, therefore, about learning from experiences, as much as learning about experiences (Gibbs, 1988; Kolb, 1984). Although reflection is known to be, at times, an imperfect means of reviewing practice, because there is always the possibility of biased reflection, or poor memory (Jones, 1995), it is a means of allowing student nurses and qualified nurses to ask questions about their practice and look at it in the light of knowledge and evidence.
If you need assistance with writing your reflective nursing essay, our professional reflective nursing essay writing service is here to help!
Find out moreUsing reflection, this essay will attempt to examine the care of an older adult with dementia, in order to examine the elements of clinical decision making and clinical reasoning in relation to their care and the management of care for them in the longer term. As such, it will also look at elements of care planning for this patient, and the processes which surrounded a key clinical decision, which is about place of care for the designated patient, who will be described below. The essay will be based within the framework of Gibbs (1988) cycle of reflection, which provides a structure and guideline for constructive reflection and allows practitioners to develop action plans for future practice improvement (see Appendix). The essay will present the case history and summary of the client’s clinical/health status, and then will follow the structure of the Gibbs (1988) reflective cycle. It will conclude with the action plan and a brief conclusion of the arguments developed throughout the essay.
Case History/Summary
The patient, whose name has been changed to protect confidentiality, is Arthur, a 69 year old man who was admitted to a general medical ward three weeks ago with pneumonia. Arthur is married to Anne, who is also 69, and both are retired teachers. Arthur was diagnosed with vascular dementia three years ago, and his health, and in particular, his symptoms of dementia, have been steadily worsening since that time. Anne is his chief carer, and gets regular support and help from their two children, a daughter, who is a full time clerical worker, and a son, who is married and lives an hour’s drive away from his parents. Anne and Arthur live in their own home, where they have lived since they were married 47 years ago.
Arthur’s symptoms are memory loss and dysfunction, apathy, fatigue, withdrawal, fixation on routines, communication difficulties, and ‘wandering’. Arthur is accustomed to regular social activities at the local Home Guard club, some of which Anne attends with him, and also to going into the local shopping area most days to buy a paper. Anne has to help him with the majority of his activities of daily living. His appetite has decreased, and he needs assistance with dressing, hygiene and other self-care activities. Anne helps him manage his medication. He has a history of essential hypertension, which is managed with anti-hypertensive medication.
Arthur developed pneumonia following a viral infection, and was admitted with dyspnoea, pyrexia and increased confusion, alongside dehydration. He was treated on a medical ward, and during this time was reviewed by an occupational therapist, social work liaison, and by the mental health team, as well as his medical team. His pneumonia responded well to antibiotic therapy, and he received nutritional supplements and assistance with some of his activities of daily living.
Reflection
Description: What Happened
Arthur’s physical health improved sufficiently for the medical team to determine that he was ready for discharge from the medical ward. Initially, the discharge plan was straightforward, and had been commenced on admission, and finalised by the nursing team looking after Arthur, under the leadership of his named nurse. Arthur was to be discharged home to his own home, with community nursing involvement. However, because of his degenerative condition, and his current state of health and wellbeing, one of the nurses on the team objected to this plan, and decided that it might be time to consider the best place of care for Arthur in the longer term. In the light of her referral to the medical consultant, and to the primary care nurse consultant, a full case conference and multidisciplinary review was called to review the discharge plan. A number of professionals were present: occupational therapy, a social worker, his named nurse, the nurse who had instigated the case conference, the Nurse Practitioner, a representative of the mental health team, and the author, along with Arthur’s Registrar and SHO.
Each professional presented their case, and discussed Arthur’s current state of health, and the support, care and input he needed. Because of his increasing debilitation, reports of his wandering behaviours on the ward, and his increasing dependence on carers, it was decided that Arthur should not be discharged home, but instead a place should be found in an EMI nursing home, where he could receive the level of support believed to be necessary for him. It was agreed that a nursing home close to his own home would be chosen, so that his wife would be able to visit him, but the home found for him was seven miles away from their home, and when his wife was informed of his place of care after discharge, she was upset. She wanted Arthur at home with her, and insisted that she could cope with his care. She also explained that the care facility they proposed was not on an easily accessible bus route, and it would take two buses and a considerable amount of time to travel from her home to visit him. Despite this, she was informed that the best place for him now was a nursing home, because his safety was at risk, and eventually, it was agreed that he be discharged to this nursing home as soon as a room became available.
Feelings: What Were You Thinking and Feeling.
My feelings were very much around empathy with Arthur’s wife, who wanted Arthur discharged to his familiar home environment, but also a sense of concern for Arthur, for his safety and wellbeing, and for the burden that his care was placing on his wife. However, I also felt quite strongly that she should have been included in the case conference. I also felt that Arthur should have been consulted about where he preferred to be discharged to. Although he had poor communication, there were times when he was able to appear at least aware of his surroundings and circumstances, and I felt that someone should have tried to get his thoughts and feelings on where he would go after discharge. I felt that the multidisciplinary team was working effectively, that they were communicating openly and professionally about the care, but that they still did not quite seem to see Arthur as a person, a whole person, with a life, a family, and his own preferences. Instead, I felt that they saw him predominantly in terms of the problems he posed for care services. And I felt that this was not necessarily the best ethos to underpin such a significant, life-changing decision.
Evaluation: What Was Good and Bad about the Experience.
Positive aspects of the experience included the insight I gained into a multidisciplinary team case conference, in which all the professionals concerned were not only well prepared and well meaning, but eager to listen to each other, to listen to people’s experiences of caring for Arthur, and to debate the whys and wherefores of his case and the discharge decision. Attitudes towards Arthur were positive, in terms of focusing on his wellbeing, safety, and prognosis, as well as focusing on the wellbeing of his wife and main carer.
However, negative aspects of this were chiefly the exclusion of Anne and Arthur from the case conference, and the lack of the presence of a member of the community nursing team, or Arthur’s GP, or anyone who actually understood his home circumstances properly. It seemed to me that no one was able to really state with certainty what his home circumstances were like. I also felt that the team should have considered the effects on Anne of ‘losing’ her husband’s presence in her home, because this could have consequences for her emotional, social and even financial wellbeing. While Arthur is their primary concern, if they had seen him and his wife in terms of the realities of their lives together, this might have affected their decision.
Analysis: What Sense Can You Make of the Situation?
Providing care for the older adult who has a diagnosis of dementia, whatever kind, is difficult and challenging, because the disorder affects so many aspects of their lives, not just their ability to take care of themselves. The NSF for Older People (DoH, 2001) clearly states that all care for the older adult should be based on person-centred care principles, looking at the individual needs, and looking at the person in context of their social life and home life. However, because the older adult is more likely to have a number of concurrent health problems (Grabbe et al, 1997), providing care to meet all the needs of the patent can be very challenging. The literature suggests that despite the Governmental guidance, and the ongoing drive to improve care for the older population, standards of care for this sector are still not as good as they should be (Helme, 2007). This suggests that there are still considerable improvements to be made in the ways that such people are cared for, and the kinds of decisions made and treatment choices offered for them (Redfern and Ross, 2001).
Dementia is a difficult disease to plan care around, because it has so many manifestations, and for different reasons. It is a very prevalent disorder in the older population (DoH, 2001). According to Helme (2007) more than 50% of elderly people in nursing homes, and an equivalent number of elderly patients who are admitted to hospitals, have dementia. This poses a considerable burden on health and social care. But the NSF also argues that it is vital that older people’s dignity is preserved and prioritised within these healthcare services (DoH, 2001), and if this is the case, then the kinds of decisions made about their place of care, as in the case of Arthur, should be decisions that are about their dignity, and their autonomy. It could be, in this case, that the balance between preserving Arthur’s autonomy at home, and between protecting his dignity (he has been known to wander out of the house in his underwear, or get lost in town), has brought the team to their decision. If the team are practising patient centred care, or person-centred care, then Arthur’s wellbeing would be the reason for the decision.
However, this is not always the case, and it could be that the decision has been made based on what is likely to cause the least amount of strain on the community health and social care services (Dellasega and Fisher, 2001). There is some evidence in the healthcare literature that many healthcare professionals continue to have innate prejudices or stereotypes of elderly patients (Gunderson et al, 2005). If this is the case, then Arthur may be being judged based on his diagnosis, and on preconceptions about his current clinical/mental state, rather than on a holistic picture of his whole life and his social context. There are those who would argue that making this decision for Arthur is the wrong course of action, because he has been functioning well at home prior to hospital admission for a medical problem, and there is no reason why he could not carry on with the same level of support for the time being (Hoare, 2004). However, it might be that this admission to hospital has been the first time that such a large team of healthcare professionals from different disciplines has had the opportunity to assess Arthur’s current health status and healthcare needs, and this is what has led to this decision (Fielo, 1998). It might be, for example, the first time the true impact of Arthur’s condition on the activities of daily living has been observed (Farley et al, 2006). However, it is also important to remember that as a patient with Dementia, Arthur is likely to behave very differently in a hospital setting than he would in a familiar home environment, and so this assessment may not be based on how he usually manages his daily life (Zarit and Zarit, 2007). However, if the professionals involved believe that the complexity of Arthur’s needs are such that the easiest place for Arthur to be cared for is within a nursing home environment (Miller et al, 1996), this might be the reason for the decision, perhaps in relation to an awareness of local resources and availability of certain support services for Arthur (Eloniemi-Sulkava et al, 2001).
The process of discharge planning is one which still seems something of a mystery, despite the clear communication between the multidisciplinary team. It is apparent from the literature on the subject that discharge planning conferences can be difficult, and for many health professionals and patients, it can be hard to get your opinion across and make sure that this opinion, or observation, is taken seriously (Efraimsson et al, 2006). Certainly, I felt that I could not voice my opinion during this conference, and yet in hindsight I feel that I should have done so, because I really feel that the most important people were missing from the case conference. The voice of Arthur was not there, perhaps because the team believed he would not be able to communicate effectively (Efraimsson et al, 2004), but Anne should definitely have been involved, as his wife and primary carer (DoH, 2001).
The literature shows that lack of involvement in discharge planning, particularly when significant decisions are being made such as this, disempowers patients and their families and can have detrimental effects on health and wellbeing (Efraimsson et al, 2003). Leaving Anne out of this decision may have an impact on her health and wellbeing, including her mental and emotional health, and if she had been involved, she might have come to the same conclusions that the team had, rather than just having them make a rather paternalistic decision without consulting her (Redfern and Ross, 2001).
Conclusion: What Else Could you Have Done?
One conclusion that I have reached through examining this case, is that it is important to question care decisions and clinical decision making processes, even if you are in the minority (Daly, 1998). In this situation, I felt disempowered, and I am sure that it might have been the case that Anne would have felt quite challenged to be part of the conference, but it should have been opened up to include her and to give her a chance to voice her own thoughts and feelings, and provide the insight into Arthur’s health, wellbeing and home life that was lacking from the conference. Another conclusion I have reached is that while multidisciplinary conferences are important, there can still be underlying personal agendas, or prejudices, and so focusing on a person-centred model of care and discharge planning is important. Also, it might be that the label of dementia has been colouring everyone’s reactions and making them lean towards nursing home care because of what they know about dementia, rather than because of what they know about Arthur. I should have raised the questions that I had, and been more proactive.
I also felt that they could have referred more explicitly to the available guidelines, such as the NSF (DoH, 2001), and the local policies and guidelines on discharge planning, and on social care planning. There should have been community nurses or Arthur’s GP involved in the discharge conference. I should have raised these points, and perhaps referred to the appropriate guidance, or asked for it.
Action Plan: If it arose again, what would you do?
- I would ensure that the patient and their primary carers were included in the discharge planning conference, that their preferences, experiences and opinions were sought, and that these were incorporated into the clinical decision making process.
- I would gather together all available policies, guidance and governance documents relating to the case. I would also seek out and gather together as much of the evidence base as possible relating to the patient’s care, in order to make a more reasoned decision.
- I would make sure that the community health professionals who had been involved in Arthur’s care up to the point of his admission to hospital were also involved in the discharge conference. This would mean that a more realistic picture of his needs was presented.
- I would include detailed information about an alternative plan of care and social support for Arthur, one which included realistic assessments of available resources and impact on current care provision.
- I would make sure that the impact of this admission on Anne and her home situation was also considered in making the final decision. I would also attempt to ensure that the discharge plan included identification and mobilisation of resources and support services for Anne as well as for Arthur.
Conclusion
It would appear from this reflection that a significant decision making process such as this, even when many good principles are adhered to, is complex and difficult, and it is important to make sure that all aspects of the client’s needs are being met, not just their safety and medical/social care needs. Decisions such as this cannot be made without the full picture and without considering alternatives to what might appear to be the easiest solution.
References
Daly, W..M. (1998) Critical thinking as an outcome of nursing education. What is it? Why is it important to nursing practice? Journal of Advanced Nursing 28 (2) 323-331.
Department of Health (2001) The National Service Framework for Older People Available from www.dh.gov.uk. Accessed 10-11-08.
Dellasega CA. Fisher KM (2001) Posthospital home care for frail older adults in rural locations. Journal of Community Health Nursing. 18(4): 247-60.
Draper, B. & Low, L. (2005). What is the effectiveness of acute hospital treatment of older people with mental disorders? International Psychogeriatrics, 17, 539-555
Efraimsson, E., Sandman, P. Hyden, L-C., and Rasmussen, B.H. (2006). How to get one’s voice heard: the problems of the discharge planning conference. Journal of Advanced Nursing 53 (6) 646-655.
Efraimsson, E., Rasmussen, B.H., Gilje, F. and Sandman, P. (2003) Expressions of power and powerlessness in discharge planning: a case study of an older woman on her way home. Journal of Clinical Nursing 12 707-716.
Efraimsson, E., Sandman, P. Hyden, L-C., and Rasmussen, B.H. (2004). Discharge planning: ‘fooling ourselves?’ – patient participation in conferences. Journal of Clinical Nursing 13 562-570.
Eloniemi-Sulkava, U., Notkola I.L., Hentinen, M. et al (2001) Effects of supporting community-living demented patients and their caregivers: a randomized trial. Journal of the American Geriatric Society 49(10):1282-7.
Farley, A., McLafferty, E. and Hendry, C. (2006) The physiological effects of ageing on the activities of living. Nursing Standard 20(45) 46-52.
Fielo, S. B. (1998) Discharge Planning for the Elderly: A Guide for Nurses. Nursing and Health Care Perspectives Volume 19(2) 94-95.
Gibbs, G. (1988) Learning by Doing. A Guide to Teaching and Learning Methods Further Education Unit, Oxford Polytechnic, Oxford
Gould, D., Berridge, E-J. And Kelly, D. (2007) The National Health Service Knoweldge and Skills Framework and its implications for continuing professional development within nursing. Nurse Education Today 27 26-34.
Grabbe, L., Demi, A., Camann, M.A. and Potter, L. (1997) The health status of elderly persons in the last year of life: a comparison of deaths by suicide, injury an natural causes. American Journal of Public Health 87 (3) 434-437.
Gunderson, A., Tomkowiak, J., Menachemi, N. and Brooks, M.D. (2005) Rural physicians’ attitudes toward the elderly: evidence of ageism? Quality Management in Health Care 14 (3) 167-176.
Hargreaves, J. (2004) “So how do you feel about that? Assessing reflective practice.” Nurse Education Today 24 (3) 196-201.
Hoare K. (2004) Care home placement: can admission direct from acute hospital be justified? Nursing Older People. 16(6): 14-17.
Jones, P.R. (1995) Hindsight bias in reflective practice: an empirical investigation. Journal of Advanced Nursing 21 (4) 783–788.
Kolb, D. A. (1984). Experiential Learning London: Prentice Hall.
Miller, J., Neelon, V., Dalton. J. et al (1996) The assessment of discomfort in elderly confused patients: a preliminary study. Journal of Neuroscience Nursing 28 (3) 175-182.
Redfern, S.J. and Ross, F.M. (2001) Nursing Older People. Third edition. Edinburgh: Churchill Livingstone.
Rolfe, G. (2005) The deconstructing angel: nursing, reflection and evidence-based practice Nursing Inquiry 12 (2), 78–86.
Zarit, S.H. and Zarit, J. M. (2007) Mental disorders in older adults–fundamentals of assessment and treatment. New York: The Guildford Press.
Gibbs (1988) Cycle of Reflection
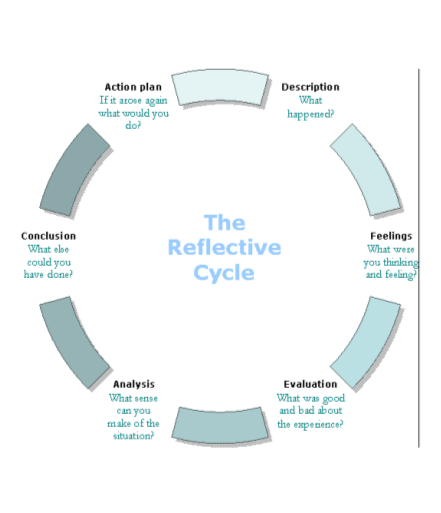
http://www.nursesnetwork.co.uk/images/reflectivecycle.gif
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "care"
Patient care is not just about the medical aspect of nursing. Patients may experience stress about their conditions, injuries, procedures, surgeries, or recovery. It is important for nurses to treat a patient's physical ailments as well as his or her emotional needs.
Related Articles

DMCA / Removal Request
If you are the original writer of this reflective essay and no longer wish to have your work published on the NursingAnswers.net website then please: